

Introduction
Alterations in the lipid spectrum are a major cause of atherosclerosis [1]. Numerous epidemiological studies have confirmed a direct link between dyslipidemia and the incidence of cardiovascular events, which are recorded both in apparently healthy individuals and in those with a history of cardiovascular disease. There is also evidence that dyslipidemia can be an independent predictor of cardiovascular events, as well as act in conjunction with other risk factors. Longitudinal studies have demonstrated the persistence of dyslipidemia throughout life, favoring the continuous progression of subclinical atherosclerosis. Scientific evidence supports the relationship between hyperlipidemia and changes in the arterial intimal layer at an early age, further strengthening the hypothesis that atherosclerosis begins early and is a chronic, progressive process [2-5]. Alterations in the lipid spectrum begin early, from childhood and adolescence, persist into youth, and clinical manifestations become apparent in adulthood [6, 7]. Dyslipidemia, particularly characterized by low levels of HDL-cholesterol (HDL-C) and elevated triglycerides (TG), is frequently observed among young people, with a prevalence ranging between 13% and 30% [8-10]. The increase in LDL-C, total cholesterol, and non-HDL-C levels observed during adolescence and youth is associated with a higher long-term cardiovascular risk [8]. Some studies conducted among young populations have shown that cumulative exposure to hyperlipidemia during youth increases the risk of developing coronary heart disease later in life, even in cases where there are only moderate increases in LDL cholesterol [9, 10]. Dyslipidemia is a modifiable cardiovascular risk factor, and early identification, along with prompt intervention, can significantly reduce overall cardiovascular risk, as well as the incidence of fatal and non-fatal events. The aim of the study was to evaluate the lipid profile in young people as an early cardiovascular risk factor.
Material and methods
The cross-sectional study was conducted on a sample of 693 apparently healthy young individuals (495 women and 198 men) aged between 17 and 30 years, who were first-year students at Nicolae Testemițanu State University of Medicine and Pharmacy (SUMF), from all integrated study programs: Medicine, Public Health, Pharmacy, and Dentistry. The study received approval from the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (Minutes no. 9 from November 20, 2012) and was carried out between September and November 2011. To analyze the lipid profile, the following parameters were assessed: total cholesterol (TC), HDL-cholesterol (HDL-C), non-HDL cholesterol (non-HDL-C), LDL-cholesterol (LDL-C), and triglycerides (TG). Venous blood was collected in the morning after at least 8 hours of fasting; the serum was separated, aliquoted, and stored at –70°C. The period before freezing did not exceed 6 hours. Serum lipids were determined in the INVITRO Diagnostics Laboratory. Tests were performed using ABBOTT Architect ci8200 equipment. Triglyceride concentration was determined using the enzymatic-colorimetric method (Triglycerides Mono SL NEW, ELITech Clinical Systems, France, and ARCHITECT Triglyceride, 7D74-21, Abbott). Total cholesterol was assessed by the enzymatic method (Cholesterol SL ELITech Clinical Systems, France, and ARCHITECT Cholesterol, 7D62-21, Abbott). HDL-cholesterol concentration was estimated by the enzymatic-spectrophotometric method with precipitation (HDL-Cholesterol ELITech Clinical Systems, France, and ARCHITECT ULTRA HDL, 3K33-21, Abbott). LDL-cholesterol content was measured directly (ARCHITECT Direct LDL, 1E31-20, Abbott). Non-HDL cholesterol was calculated using the formula: non-HDL-C = TC – HDL-C (mmol/l) [11]. The evaluation of changes in the lipid spectrum was carried out according to the recommendations of the European Society of Cardiology and the National Clinical Protocol for Dyslipidemias [12, 13] (Table 1).
Table 1. Threshold values for interpretation of lipid parameters (mmol/l) | |||||
| TC | LDL-C | HDL-C | non-HDL-C | TG |
| Normal level | < 5.0 | < 2.6 | ≥ 1.0* ≥ 1.3** | < 3.8 | < 1.7 |
| Modified level | ≥ 5.0 | ≥ 2.6 | < 1.0* < 1.3** | ≥ 3.8 | ≥ 1.7 |
Note: * – men; ** – women;. TC – total cholesterol; LDL-C – LDL-cholesterol; HDL-C – HDL-cholesterol; non-HDL-C – non-HDL cholesterol; TG – triglycerides. | |||||
The R programming environment was used to calculate the statistical parameters, employing the EpiTool applications [14-16]. The differences between the statistically significant mean values (p < 0.05) and their 95% confidence intervals were calculated.
Results
The stratified analysis of the lipid profile of the evaluated young people showed that total cholesterol (TC) values ranged from 1.71 to 6.89 mmol/l, with a mean value of 3.89 ± 0.845 mmol/l. In men, TC ranged from 1.88 to 6.89 mmol/l, and in women from 1.71 to 6.52 mmol/l (p = 0.5239). The mean value of TC was higher in women (3.90 ± 0.855 mmol/l) than in men (3.85 ± 0.845 mmol/l) (p = 0.4354). Mean HDL cholesterol (HDL-C) was 1.22 ± 0.328 mmol/l, with a range between 0.53 and 2.80 mmol/l. HDL-C values ranged from 0.57 to 2.01 mmol/l in men and from 0.53 to 2.80 mmol/l in women (p = 0.0068). In women, the mean HDL-C value was higher (1.26 ± 0.337 mmol/l) compared to men (1.14 ± 0.328 mmol/l), the difference being statistically significant (p = 3.56×10⁻⁶). Non-HDL cholesterol (non-HDL-C) in the study group had a mean value of 2.66 ± 0.718 mmol/l, with limits ranging from 0.62 to 5.76 mmol/l. In men, non-HDL-C values ranged from 1.18 mmol/l to 5.76 mmol/l, while in women from 0.62 mmol/l to 4.92 mmol/l (p = 0.2885). Mean non-HDL-C was higher in men (2.70 ± 0.685 mmol/l) than in women (2.65 ± 0.731 mmol/l) (p = 0.334). The LDL-cholesterol (LDL-C) content ranged from 0.30 to 5.04 mmol/l, with a mean value of 1.94 ± 0.787 mmol/l. LDL-C values ranged from 0.47 mmol/l to 5.04 mmol/l in men and from 0.62 mmol/l to 4.92 mmol/l in women (p = 0.1304). The mean LDL-C was higher in men (2.00 ± 0.787 mmol/l) compared to women (1.92 ± 0.807 mmol/l) (p = 0.2079). Triglyceride (TG) concentration ranged from 0.18 mmol/l to 7.16 mmol/l, with a mean value of 1.16 ± 0.572 mmol/l. In women, TG values ranged from 0.24 mmol/l to 7.16 mmol/l and from 0.18 mmol/l to 5.24 mmol/l in men (p = 0.130). Mean TG content was significantly higher (p = 0.0042) in men (1.26 ± 0.572 mmol/l) than in women (1.13 ± 0.586 mmol/l) (Table 2).
Table 2. Comparative characteristics of lipid parameters (n = 693). | ||||||
Statistical parameter | Sex | TC mmol/l | HDL-C mmol/l | non-HDL-C mmol/l | LDL-C mmol/l | TG mmol/l |
Range of variation | Total | 1.71–6.89 | 0.53–2.80 | 0.62–5.76 | 0.30–5.04 | 0.18–7.16 |
M | 1.88–6.89 | 0.57–2.01 | 1.18-5.76 | 0.47–5.04 | 0.18–5.24 | |
F | 1.71–6.52 | 0.53–2.80 | 0.62–4.92 | 0.30-3.97 | 0.24–7.16 | |
Median | Total | 3.96 | 1.19 | 2.69 | 2.03 | 1.27 |
M | 3.99 | 1.11 | 2.75 | 2.06 | 1.32 | |
F | 3.95 | 1.21 | 2.64 | 2.00 | 1.24 | |
Mean ± SD | Total | 3.89 ± 0.845 | 1.22 ± 0.328 | 2.66 ± 0.718 | 1.94 ± 0.787 | 1.16 ± 0.572 |
M | 3.85 ± 0.845 | 1.14 ± 0.328 | 2.70 ± 0.685 | 2.00 ± 0.787 | 1.26 ± 0.572 | |
F | 3.90 ± 0.855 | 1.26 ± 0.337 | 2.65 ± 0.731 | 1.92 ± 0.807 | 1.13 ± 0.586 | |
| t-test p value | -0.7808 0.4354 | -4.698 3.56 × 10-6 | 0.9666 0.3344 | 1.2615 0.2079 | 2.8779 0.0042 |
| F-test p value | 0.9244 0.5239 | 0.7162 0.0068 | 0.8782 0.2885 | 0.8309 0.1304 | 0.7964 0.0633 |
Note: n(M) = 198 –number of men. n(F) = 495 –number of women. TC – total cholesterol; LDL-C – LDL-cholesterol; HDL-C – HDL-cholesterol; non-HDL-C – non-HDL cholesterol; TG – triglycerides. Statistical significance was set at p < 0.05. The t-test was applied to assess differences between mean values; F-test was applied to assess differences in variance between datasets. | ||||||
The majority of the evaluated young people (91.8%) had TC values within normal limits (less than 5.0 mmol/l), while 8.2% had levels above the threshold considered normal. Among women, the proportion of those with TC above the threshold value was 9.3%, and among men, 5.6% (p = 0.106). It is important to note that more than half of the participants (52.5%) had HDL-C values below the gender-specific thresholds. Thus, 58.8% of the women had HDL-C levels ≤ 1.29 mmol/l, and 36.9% of the men had levels ≤ 1.03 mmol/l. The association between HDL-C and gender was statistically significant ((χ² = 27.249, p=5 × 10-4). Non-HDL-C concentrations were within normal limits (≤ 3.8 mmol/l) in 94.1% of participants, and 5.9% were above the reference threshold. Analysis by gender revealed elevated non-HDL-C levels in 6.7% of women and 4.0% of men (p = 0.218). Also, LDL-C remained within normal limits (≤ 2.59 mmol/l) in 78.6% of participants, while 21.4% had values above the recommended threshold. According to gender, 22.2% of men and 21.0% of women had elevated LDL-C values, with no statistically significant difference between the two groups (p = 0.779). Regarding TG, 91.8% of participants had levels within normal limits (< 1.7 mmol/l), while 8.2% had values above the threshold. Elevated TG levels were observed in 8.7% of women and 7.1% of men (p = 0.528) (Fig. 1). Therefore, the comparative analysis of the lipid profile according to sex revealed a statistically significant difference only for HDL-C (χ² = 27.249, p = 5× 10-4). The proportion of women with pathological HDL-C levels (≤ 1.29 mmol/l) was significantly higher (58.8%) compared to men (36.9%). For the other parameters (TC, LDL-C, non-HDL-C, and TG), sex differences were not statistically significant (Fig. 1).
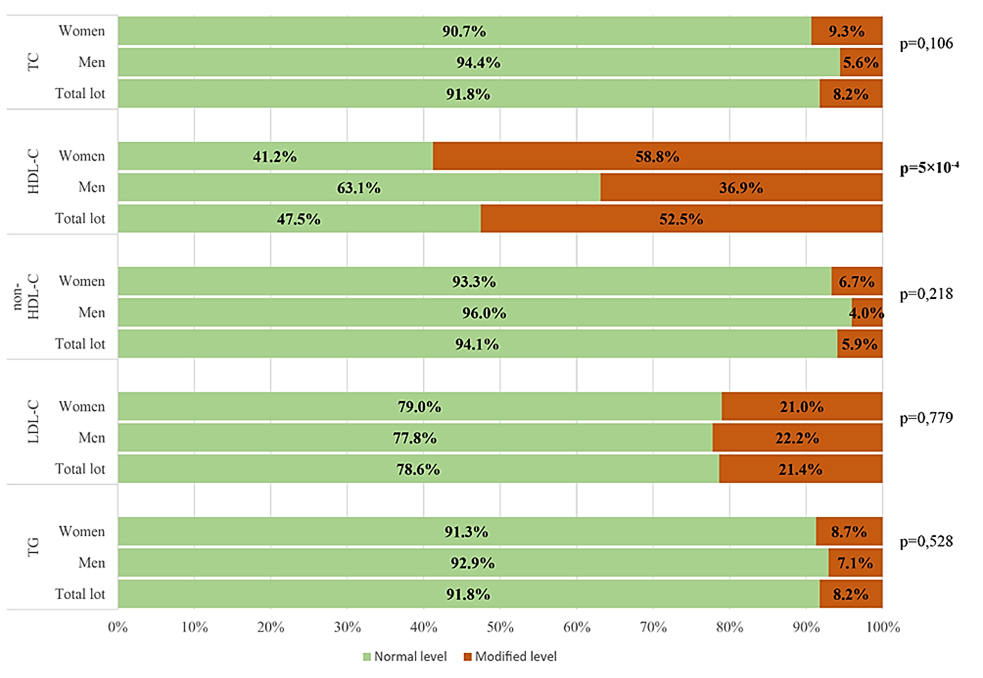 |
Fig. 1 Frequency of lipid parameter levels in relation to threshold values (mmol/l) Note: TC – total cholesterol; LDL-C – LDL-cholesterol; HDL-C – HDL-cholesterol; non-HDL-C – non-HDL cholesterol; TG – triglycerides. Normal level – the percentage of subjects with the parameter within normal limits; Modified level – the percentage of subjects with values above the threshold (TC; LDL-C; non-HDL-C; TG) and below the sex-specific threshold (HDL-C). p < 0.05 was considered statistically significant. |
Discussion
The results of our study, using threshold values for lipid parameters [12, 13], revealed a relatively high prevalence, with more than half (52.5%) of the young assessed individuals having HDL-C levels below gender-specific thresholds. Low HDL-C levels among youth have also been documented in international research on this age group, with a prevalence ranging from 13% to 30% [9, 17, 18]. Our study recorded HDL-C levels below gender-specific threshold values in 58.8% of women and 36.9% of men, with a statistically significant difference (p = 5×10-4). Other research conducted in the same age group demonstrated the presence of this risk factor in 18.2% of men and 8.1% of women [17]. More comprehensive data are provided by a large-scale study from China involving 22,379 young students, which reported a high proportion (74%) of individuals with low HDL-C levels, particularly among men (23% vs. 7.2% in women). Elevated triglycerides (14.5%) were also noted, but as in our research, other risk factors such as diet, physical activity level, and age-specific hormonal characteristics were not analyzed [10]. A study conducted among medical students in Sri Lanka highlighted numerous deviations in the lipid profile among young people, including a prevalence of hypercholesterolemia of 25.4% and hypertriglyceridemia of 5.3%. The authors reported that these abnormalities were significantly more frequent among men (12.3%) compared to women (1.6%), with the difference being statistically significant (p = 0.006). Additionally, low HDL-C levels were observed in approximately 31.6% of participants, while 12.2% had elevated LDL-C values [19]. Several local studies among young medical students have likewise demonstrated changes in lipid profile parameters. Thus, a cross-sectional study conducted on a sample of 456 students from the Nicolae Testemițanu State University of Medicine and Pharmacy revealed alterations in the lipid profile in 52.0% of participants, of whom 40.9% had HDL-C values below gender-specific reference thresholds, 11.8% had hypertriglyceridemia, and 7.3% had hypercholesterolemia [20]. Another study conducted among students at the same institution reported a prevalence of 53.0% for at least one altered lipid parameter among 302 women. Within this sample, 34.1% of participants had low HDL-C levels, 13.6% had hypertriglyceridemia, and 14.2% had hypercholesterolemia, while 7.0% exhibited elevated non-HDL-C values [21]. At the same time, among men, at least one altered lipid parameter was identified in 34.0% of 138 medical students, with low HDL-C being the most frequently observed abnormality [22]. These data confirm the trend observed in our own analysis, suggesting a significant frequency of dyslipidemia among the young population.
In comparison, data from the STEPS studies conducted in the Republic of Moldova indicate that, among the general population aged 18 to 29, 17.8% of young people had mean total cholesterol (TC) values above 5.0 mmol/l. The differences between sexes were statistically significant, with a higher prevalence in women (20.0%) compared to men (15.5%) [23, 24]. The changes observed in the lipid profile may potentially be influenced by genetic factors, considering the concept that genetic factors shape individuals' health status in youth, while behavioral and environmental factors become more significant with age – a point that should be taken into account when developing personalized preventive strategies.
Conclusion
The study demonstrated that more than half of the young individuals (52.5%) had HDL-C levels below gender-specific thresholds. These changes in the lipid profile increase the atherogenic potential of plasma, highlighting the importance of implementing early preventive measures in this age group. In this context, it is essential to expand the use of cardiovascular risk assessment tools among the young population.
Competing interests
None declared.
Authors’ contributions
All authors contributed equally to the conduct of the study and the drafting of the manuscript. All authors reviewed the work critically and approved the final version of the manuscript.
Informed consent for publication
Obtained.
Acknowledgements and funding
The current study is an integral part of the institutional projects no. 11.817.09.21A, 2011-2014 "Molecular Genetic Polymorphism of Metabolic Cardiovascular Risk Factors in Young People", and no. 15.817.04.42A, 2015-2018 "Identification and Validation of Genetic and Epigenetic Biomarkers in Chronic Non-Communicable Diseases with Major Impact on Public Health".
The group of authors expresses deep gratitude to the University Primary Health Care Clinic of Nicolae Testemițanu State University of Medicine and Pharmacy and INVITRO Diagnostics Laboratory for their support in generating the lipid profile data.
Ethics approval
The study protocol was approved by the Research Ethics Committee of the Nicolae Testemițanu State University of Medicine and Pharmacy (Minutes no. 9, dated November 20, 2012).
Provenance and peer review
Not commissioned, externally peer-reviewed.
Authors’ ORCID IDs
Diana Chiosa – https://orcid.org/0000-0002-3652-8021
Rodica Ignat – https://orcid.org/0000-0002-4934-8820
Alexei Levițchi – https://orcid.org/0000-0003-1784-654X
Ghenadie Curocichin – https://orcid.org/0000-0003-0613-4360
References
Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies with the special contribution of the European Association of Preventive Cardiology (EAPC). Eur Heart J. 2021;42(34):3227-3337. doi: 10.1093/eurheartj/ehab484.
Palacio-Portilla EJ, Roquer J, Amaro S, Arenillas JF, Ayo-Martín O, Castellanos M, et al. Dyslipidemias and stroke prevention: recommendations of the Study Group of Cerebrovascular Diseases of the Spanish Society of Neurology. Neurología (English Ed.). 2022;37(1):61-72. doi: 10.1016/j.nrleng.2020.07.021.
Zokaei A, Ziapour A, Khanghahi ME, Lebni JY, Irandoost SF, Toghroli R, et al. Investigating high blood pressure, type-2 diabetes, dislipidemia, and body mass index to determine the health status of people over 30 years. J Educ Health Promot. 2020;9(1):333. doi: 10.4103/jehp.jehp_514_20.
Orozco-Beltran D, Gil-Guillen VF, Redon J, Martin-Moreno JM, Pallares-Carratala V, Navarro-Perez J, et al. Lipid profile, cardiovascular disease and mortality in a Mediterranean high-risk population: the ESCARVAL-RISK study. PloS One. 2017;12(10):e0186196. doi: 10.1371/journal.pone.0186196.
Sadeghi M, Golshahi J, Talaei M, Sheikhbahaei E, Ghodjani E, Mansouri M, et al. 15-year lipid profile effects on cardiovascular events adjusted for cardiovascular risk factors: a cohort study from Middle-East. Acta Cardiol. 2021;76(2):194-199. doi: 10.1080/00015385.2020.1717096.
Teo KK, Rafiq T. Cardiovascular risk factors and prevention: a perspective from developing countries. Can J Cardiol. 2021;37(5):733-743. doi: 10.1016/j.cjca.2021.02.009.
Truthmann J, Schienkiewitz A, Kneuer A, Du Y, Scheidt-Nave C. Tracking of serum lipids from prepuberty to young adulthood: results from the KiGGS cohort study. Lipids Health Dis. 2024;23(1):421. doi: 10.1186/s12944-024-02409-1.
Kiechl SJ, Staudt A, Stock K, Gande N, Bernar B, Hochmayr C, et al. Predictors of carotid intima‐media thickness progression in adolescents - the EVA‐Tyrol study. J Am Heart Assoc. 2021;10(18):e020233. doi: 10.1161/JAHA.120.020233.
Navar-Boggan AM, Peterson ED, D'Agostino RB Sr, Neely B, Sniderman AD, Pencina MJ. Hyperlipidemia in early adulthood increases long-term risk of coronary heart disease. Circulation. 2015;131(5):451-458. doi: 10.1161/CIRCULATIONAHA.114.012477.
Liu LY, Aimaiti X, Zheng YY, Zhi XY, Wang ZL, Yin X, et al. Epidemic trends of dyslipidemia in young adults: a real-world study including more than 20,000 samples. Lipids Health Dis. 2023;22(1):108. doi: 10.1186/s12944-023-01876-2.
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS guidelines for the management of dyslipidaemias. Rev Esp Cardiol (English ed.). 2017;70(2):115. doi: 10.1016/j.rec.2017.01.002.
Ministry of Health of the Republic of Moldova; Ivanov V, Dumanschi C. Dislipidemiile: protocol clinic naţional (PCN-78) [Dyslipidemias: national clinical protocol]. Chisinau: The Ministry; 2017. Romanian.
Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk: the Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur Heart J. 2020;41(1):111-188. doi: 10.1093/eurheartj/ehz455.
Wickham H. Reshaping data with the reshape package. J Stat Softw. 2007;21:1-20. doi: 10.18637/jss.v021.i12.
Wickham H. Ggplot2: elegant graphics for data analysis. 2nd ed. Dordrecht: Springer; 2009. 277 p. doi: 10.1007/978-0-387-98141-3.
Begum GS, Adari P, Manjunatha G, Kore SE, Eshwaret MD. A study of diagnostic parameters in assessment of metabolic syndrome (MetS) among medical students. Biomedicine. 2022;42(6):1361-1367. doi: 10.51248/.v42i6.1822.
Abuzhalihan J, Wang YT, Adi D, Ma YT, Fu ZY, Yang YN, et al. Prevalence of dyslipidemia in students from Han, Uygur, and Kazakh ethnic groups in a medical university in Xinjiang, China. Sci Rep. 2019;9(1):19475. doi: 10.1038/s41598-019-55480-5.
Senevirathne T, Samaranayake D, Ojithmali M, Wickramarachchi P, Weerasinghe A, Muthuthamby MM, et al. Cardio-metabolic risk among undergraduate medical students of a selected Faculty of Medicine in Colombo. Res Square. 2020 March 26. doi: 10.21203/rs.3.rs-19253/v1.
Gavriliuc S, Ignat R, Levitchi A, Lupu L, Chiosa D, Buza A, et al. Prevalence of lipid abnormalities among young Moldovans. In: MedEspera: 6th International Medical Congress for Students and Young Doctors; 2018 Mai 12-14; Chişinău, Republic of Moldova: abstract book. Chișinău: [s. n.]; 2016. p. 53-54.
Gavriliuc S. The rate of obesity and dyslipidaemia among young moldovan women. In: MedEspera: 7th International Medical Congress for Students and Young Doctors, 2018 Mai 3-5; Chişinău, Republic of Moldova. Chisinau; 2018. p. 92.
Gavriliuc S, Buza A, Butovscaia C, Istrati V. Silent cardiovascular risk factors among medical students. Mold Med J. 2021;64(1): 41-44. doi: 10.5281/zenodo.4527088.
World Health Organization (WHO). Prevalence of noncommunicable disease risk factors in the Republic of Moldova: STEPS 2013. Copenhagen: WHO Regional Office for Europe; 2014. 220 p.
World Health Organization (WHO). Noncommunicable diseases: progress monitor 2022 Geneva: WHO regional Office for Europe; 2022. 225 p.