

Introduction
The aberrant right subclavian artery (ARSA) was first discovered by Hunauld in the 18th century during an autopsy and represents the most common congenital anomaly of the aortic arch, with an incidence of 0.5-1.0% in the general population [1, 2]. The clinical importance of ARSA stems from its potential to cause symptoms through compression of adjacent mediastinal structures, primarily the esophagus, and a tendency to aneurysmal degeneration (Kommerell diverticulum). When esophageal compression by an ARSA leads to difficulty swallowing, the condition is referred to as “dysphagia lusoria” (from the Latin term “lusus naturae” – freaks of nature), a term introduced by Bayford in 1794 [1, 3, 4]. Since most individuals (more than 90%) with ARSA remain asymptomatic or undiagnosed with this anomaly throughout their lives, there is a paucity of data regarding the management of symptomatic cases. Current literature mostly includes case reports and case series, with significant heterogeneity of clinical presentations, diagnostic modalities, and curative approaches.
Clinical case
We report the clinical case of a 54-year-old female patient who presented to the outpatient clinic of the Division of Thoracic Surgery, complaining of progressive dysphagia, fatigue, and morning cough. The anamnesis also revealed two episodes of black-colored stools and a sensation of compression localized at the lower cervical level, with subsequent radiation to the thoracic region. The patient described a gradual onset of dysphagia approximately 6 months prior to presentation. These symptoms had been gradually worsening over the past month, especially after eating, particularly with solid and semi-liquid foods. Importantly, the patient reported an unintentional weight loss of approximately 8 kilograms over the past few months, attributed to reduced oral intake and food avoidance due to dysphagia. The patient was examined in several outside medical institutions with suspicion of malignancy, neurological, or even psychiatric diseases, none of which were confirmed.
The patient's past medical history includes chronic autoimmune thyroiditis (Hashimoto's) diagnosed approximately 10 years ago, stage II arterial hypertension, NYHA class II chronic heart failure, and grade I axial hiatal hernia associated with gastroesophageal reflux disease. The initial physical examination did not reveal cervical deformities, noting only the presence of slightly enlarged bilateral submandibular lymph nodes. The thoracic region showed no visible abnormalities. The patient denied any history of bodily injuries or trauma.
During the initial hospitalization, paraclinical investigations revealed microcytic hypochromic anemia (hemoglobin 88.0 g/L, erythrocytes 5.16 × 1012/L, hematocrit 33.5%), associated with mild leukopenia (leukocytes 3.60 × 109/L). The blood coagulation test and biochemistry profile were within the normal range.
Ultrasonography of the cervical region showed a normal sonographic appearance of the musculo-tendinous, cutaneous, and subcutaneous structures, along with bilateral submandibular lymphadenopathy with ganglion hyperplasia up to 20 × 8 mm and findings suggestive of chronic autoimmune thyroiditis (Hashimoto's).
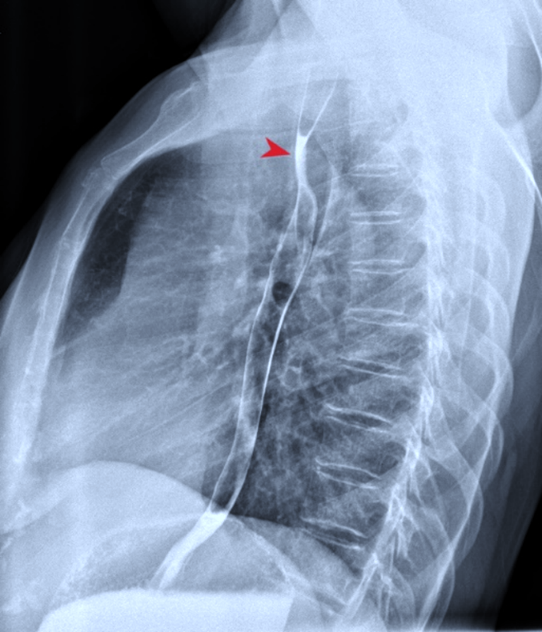
The presence of anemia, weight loss, and black-colored stool initially raised clinical suspicion for upper digestive tract pathology, and esophagogastroscopy was attempted. However, the procedure was stopped at the level of the first physiological narrowing of the esophagus, as the endoscope (with external diameter of 0.9 cm) could not be advanced further. Fibrobronchoscopy did not reveal any endobronchial pathologies. Barium swallow demonstrated evident esophageal narrowing at the level of Th3-Th4 vertebrae, with retention of the contrast media, suggestive of significant extrinsic esophageal compression (Fig. 1).
|
Fig. 1. Preoperative barium swallow image showing external compression of the esophagus at the T3-T4 vertebrae level. Note: The arrow indicates the level of esophageal compression. |
Computed tomography angiography with intravenous contrast (100 ml Iodixanol) identified an aortic arch anomaly – ARSA (diameter at the origin of 17 mm), originating distal to the left subclavian artery from the posterior surface of the aorta (Fig. 2) and passing to the right behind the esophagus, which was compressed between the artery and the trachea (Fig. 3). The presence of the common origin of the right and left carotid arteries – the so-called “bicarotid trunk” – and dextroposition of the thoracic lymphatic duct was also noted on the axial imaging. No other abnormalities were identified.
Cardiac ultrasonography revealed induration of the ascending aorta and the aortic and mitral valves, moderate dilation of the left atrium, and mild dilation of the right atrium, impaired left ventricular myocardial relaxation, with an ejection fraction of 63%, grade II mitral, grade I-II tricuspid, and grade I aortic insufficiency, along with signs of mild pulmonary hypertension (PASP 34 mmHg). Duplex ultrasonography of the extracranial vessels demonstrated non-diseased common and internal carotid arteries, a decreased diameter and moderate kinking of the right vertebral artery, with a peak systolic velocity of 60-70 cm/sec.
|
Fig. 2 Computed tomography angiography of the aortic arch and supra-aortic trunks. Note: bicarotid trunk (1) and aberrant right subclavian artery (2), Kieffer type III. |

Based on the results of clinical and paraclinical evaluation, the patient was diagnosed with esophageal obstruction (dysphagia lusoria) caused by ARSA type III Kieffer, with a Kommerell diverticulum, and was scheduled for surgical intervention. After a multidisciplinary discussion of possible treatment options, the decision was made to perform a right subclavian-carotid transposition surgery via a sternotomy approach.
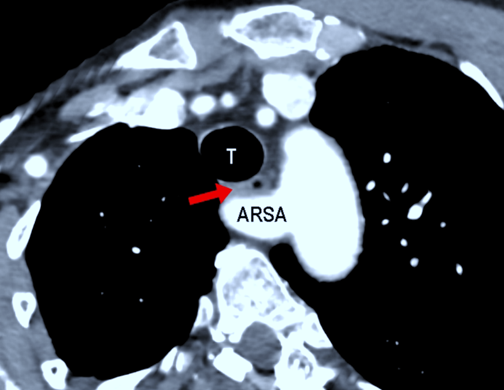 |
Fig. 3 Computed tomography angiography: compression of the esophagus between the aberrant right subclavian artery (ARSA) and the trachea (T). Note: The arrow indicates the esophageal compression. |
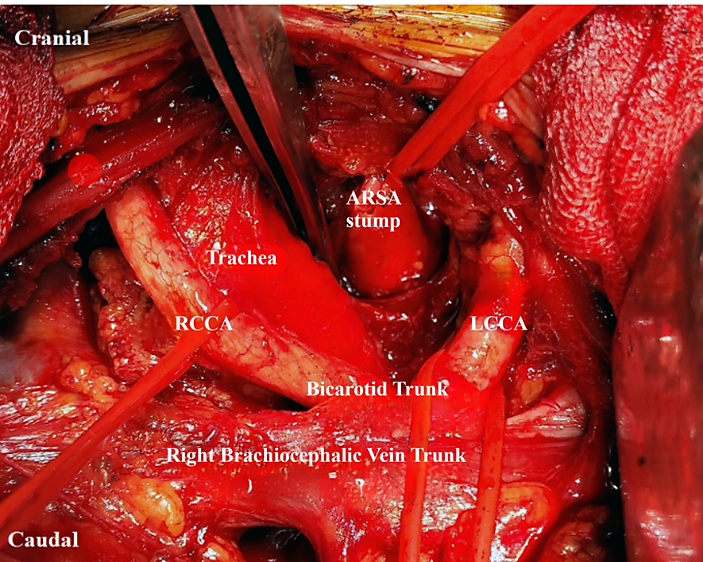
Under general anesthesia with orotracheal intubation, a median sternotomy was performed, the thoracic cavity was explored, and the aortic arch and supra-aortic trunks were carefully dissected and controlled. The ARSA, originating from the posterior surface of the aorta in Ishimaru zone 3, was identified, mobilized in the para-tracheal and para-esophageal space, and followed down to the aorta. After systemic heparinization, the ARSA trunk (Kommerell diverticulum) was slowly double-clamped as close to the aorta as possible and transected, with suture-ligation of the proximal stump using 4/0 polypropylene suture, achieving a leak-proof closure with no bleeding noted (Fig. 4).
|
Fig. 4 Intraoperative image: surgically dissected supra-aortic trunks, suture-ligated proximal stump of the transected ARSA. Note: ARSA – aberrant right subclavian artery; RCCA – right common carotid artery; LCCA – left common carotid artery. |
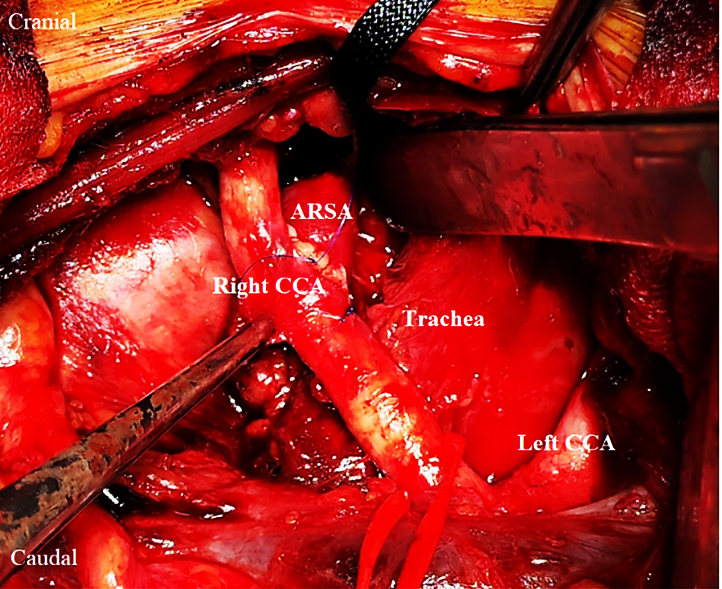
The distal segment of the ARSA, situated between the esophagus and thoracic vertebrae, was gradually dissected, retracted to the right side of the trachea, and transposed towards the right common carotid artery, avoiding any redundancy or kinks. After clamping of the right common carotid artery, an arteriotomy was performed, and an end-to-side anastomosis with the transposed ARSA was performed using a running 5/0 polypropylene suture (Fig. 5). After clamp removal, pulsatile flow was present distal to the suture line. Surgical hemostasis was achieved, and a retrosternal drain was placed, followed by sternal wound closure in anatomical layers. The surgical intervention lasted 195 minutes, with an estimated blood loss of 600 ml.
The postoperative course was satisfactory, with no clinically relevant complications. The patient was mobilized early, resumed oral intake gradually, and demonstrated progressive improvement in swallowing function. She was discharged on the 12th postoperative day in satisfactory condition, reporting the complete resolution of dysphagia symptoms with liquid and solid food.
At the three-month follow-up, the patient reported a weight gain of 5 kilograms, reflecting improved nutritional status and confirming the favorable clinical outcome. She was able to consume solid foods without pain or difficulty during swallowing, and no residual compressive symptoms were reported. Upper digestive tract endoscopy and barium swallow confirmed the normal permeability of the esophagus and excluded any pathology of the stomach and duodenum.
|
Fig. 5 Intraoperative image: end-to side anastomosis between the transposed ARSA and the right common carotid artery. Note: ARSA – aberrant right subclavian artery; Right CCA – right common carotid artery; Left CCA – left common carotid artery. |
Discussion
This review aims to synthesize the current evidence available primarily through the PubMed database concerning the anatomical variations, prevalence, diagnostic approaches, and management strategies in patients with ARSA and dysphagia lusoria.
The relationship of the ARSA to the esophagus and trachea during its mediastinal transit is clinically crucial. The most frequent course, observed in approximately 80-83% of cases, is retroesophageal, where the artery passes posterior to the esophagus, potentially compressing it against the trachea [5-7]. Less commonly – in approximately 15-17% of cases – the artery passes between the esophagus and the trachea (so-called interesophageotracheal course), compressing the esophagus against the vertebral bodies. Rarely, in around 5% of cases, ARSA may travel anterior to the trachea (pretracheal course) [8]. Imaging studies using CT have shown that ARSA is typically located anterior to the first to fourth thoracic vertebral bodies [9].
Several classification systems exist to describe the anatomic variability of the ARSA, though they are not universally applied. The Adachi and Williams classification describes subtypes based on associated branching patterns of the supra-aortic trunks [10]:
Type G-1: ARSA present as the last aortic arch branch, with normal origins for the right common carotid, left common carotid, and left subclavian arteries;
Type CG-1: Similar to G-1, but with the left vertebral artery originating directly from the aortic arch;
Type H-1: ARSA as the last branch, associated with a bicarotid trunk (common origin for both common carotid arteries);
Type N-1: Mirror image of G-1, with a right-sided aortic arch and an aberrant left subclavian artery.
Variations in the ARSA origin from the arch (superior-posterior vs. inferior-posterior) and significant variability in the luminal diameter of the ARSA have also been reported, with some cases exhibiting unusually narrow lumens [11].
In 1994, Kieffer et al. proposed a more clinically oriented classification system for ARSA, aimed at guiding surgical strategy in symptomatic patients. Summarizing their experience with surgical interventions in thirty-three adult patients with ARSA, the authors described four types of pathology [12].
Kieffer type I: non-stenotic and non-aneurysmal ARSA causing exclusively compressive symptoms;
Kieffer type II: presence of stenosis or occlusion of non-aneurysmal ARSA;
Kieffer type III: aneurysm of the origin of ARSA (Kommerell diverticulum) without aortic involvement;
Kieffer type IV: Kommerell diverticulum associated with aneurysmal dilatation of the aorta.
Associated anomalies
ARSA frequently coexists with other anatomical variations or anomalies, which can have significant clinical implications.
Kommerell diverticulum. This is an aneurysmal dilatation or outpouching at the origin of the ARSA from the descending aorta [1, 4]. The presence of a Kommerell diverticulum is clinically significant, as it may increase the likelihood and severity of compressive symptoms (dysphagia, dyspnea) and carries a risk of aneurysmal degeneration, dissection, or rupture, particularly if the diameter exceeds certain thresholds (often cited as 3-5 cm) [10].
Non-recurrent inferior laryngeal nerve. A strong association exists between ARSA and a non-recurrent course of the right inferior laryngeal nerve [1, 13, 14]. Reports suggest this occurs in up to 87% of ARSA cases. Awareness of this association is critical during thyroid, parathyroid, esophageal, or neck surgeries to prevent nerve injury [15, 16].
Bicarotid trunk. This anomaly involves a common origin for the right and left common carotid arteries directly from the aortic arch [1, 13]. It is reported to coexist with ARSA in a significant minority of cases (19.2% in one review) [13]. The presence of a bicarotid trunk alongside ARSA may increase the likelihood of dysphagia, possibly by limiting the anterior displacement of the trachea and esophagus, thus exacerbating the posterior compression by the ARSA.
Chromosomal abnormalities and syndromes. There is a well-established increased frequency of ARSA in individuals with certain chromosomal abnormalities, particularly Trisomy 21 (Down syndrome) and Trisomy 18 (Edwards syndrome) [17, 18]. Prevalence in Down syndrome has been reported as high as 26-35%.
ARSA is consistently cited as the most common congenital anomaly of the aortic arch [1, 2]. Reported prevalence figures in the general population typically range from 0.5% to 2.0% [4-7], although some sources cite wider ranges up to 4.4% [19, 20]. Specific studies provide context to these figures:
CTA studies. Large retrospective analyses of adult chest CTA scans consistently report prevalence figures around 0.5%. For instance, one study found ARSA in 32 out of 6833 patients (0.47%), and another identified 17 cases in 3460 patients (0.49%) [21].
Fetal ultrasound studies. Prenatal screening studies report prevalence rates often around 1% or slightly higher. One study detected ARSA in 20 of 1913 second-trimester fetuses (1.04%), while another found an incidence of 0.6% in 3266 fetal sonographies. Feasibility of ultrasound detection is high, estimated at 85-95% depending on trimester and factors like operator experience and maternal habitus.
Specific populations. Studies focusing on patients with known arteriopathies found a prevalence of 2.4%. As mentioned, prevalence is significantly higher in populations with Down syndrome or 22q11.2 deletion [6].
The observed variation in prevalence likely reflects differences in study methodology, population characteristics, and the sensitivity of the detection method used. CTA in adults provides a reliable estimate for that demographic, likely around 0.5%. Fetal ultrasound identifies cases early, potentially including those that remain asymptomatic, with a rate of around 1%. Cadaveric studies provide anatomical confirmation, though results may vary depending on the studied population. The increasing use and sensitivity of imaging modalities, particularly prenatal ultrasound, may lead to more frequent identification of ARSA [15], raising important questions regarding the natural history and clinical significance of incidentally or prenatally detected cases. Several studies suggest a female predominance for ARSA, with reported female-to-male ratios ranging up to 2:1 or 3:1 in some series [22].
Traditional open surgical interventions for symptomatic ARSA. Open surgical repair is the traditional approach for treating symptomatic ARSA and remains indicated for specific patient groups. The primary indication is the presence of significant symptoms, particularly dysphagia that is severe, persistent, progressive, unresponsive to conservative management, or associated with significant weight loss or nutritional compromise [23]. Other compressive symptoms, like severe dyspnea or cough, may also warrant intervention.
Anatomical factors are also crucial indications for open repair. The presence of aneurysmal dilatation of the ARSA itself often necessitates surgical intervention, even in asymptomatic patients, due to the risk of rupture, dissection, or thromboembolism [16]. While the exact size threshold for prophylactic repair of asymptomatic Kommerell diverticulum remains debated, diameters exceeding 3 cm or 5.0-5.5 cm are often cited as indications, particularly in low-risk patients.
The presence of concomitant thoracic aortic aneurysm or dissection involving the ARSA origin also typically requires open surgical management. Symptomatic occlusive disease of the ARSA, leading to arm claudication or ischemia, is another indication for intervention, usually involving revascularization. Open repair may also be preferred over endovascular options when significant esophageal or tracheal compression is the primary symptom, as endovascular exclusion alone may not relieve the mass effect [24].
Surgical approaches. Several open surgical approaches have been described, each with advantages and disadvantages, largely dictated by the specific anatomy and the goals of the operation.
Thoracotomy
Left Posterolateral Thoracotomy: Historically considered the standard approach, especially by Gross, who first described surgical correction [13]. It provides excellent exposure of the ARSA origin from the descending aorta, facilitating secure ligation or division, particularly when a Kommerell diverticulum is present or the origin is dilated [25]. However, performing revascularization (reimplantation or bypass) from this approach can be technically challenging due to the distance to suitable inflow sources, like the ascending aorta or right carotid artery.
Right Thoracotomy: Offers better access for anastomosing the distal ARSA to the right common carotid artery or ascending aorta, either directly or with an interposition graft [4]. It may provide less optimal exposure of the ARSA origin, potentially increasing the risk of leaving a residual stump if ligation is not performed flush with the aorta, which could lead to persistent symptoms or thrombosis. This approach is preferred by some for pediatric patients due to better overall exposure in smaller chests. It is also the typical approach for patients with a right-sided aortic arch and an aberrant left subclavian artery [25]. Thoracotomy is generally more invasive than cervical approaches, involving muscle division, potential rib spreading, and longer recovery times [22, 24].
Median sternotomy. This approach provides excellent access to the ascending aorta and brachiocephalic vessels, making it suitable for reimplanting the ARSA onto the ascending aorta or performing bypasses from it. However, exposure of the posteriorly located ARSA origin on the descending aorta for ligation or division can be difficult from this anterior approach.
Supraclavicular (cervical) approach. This is the least invasive of the open approaches, avoiding entry into the thoracic cavity [10, 22]. It provides good access to the distal ARSA in the neck for transposition or bypass to the right common carotid artery. It is generally considered suitable for uncomplicated, non-aneurysmal ARSA. However, this less traumatic approach is not suitable for patients with aneurysmal dilatation of the ARSA and those with dysphagia lusoria (as in our case), because the origin of the anomalous subclavian artery can be securely suture-ligated only via thoracotomy.
Hybrid and endovascular management. Development and implementation of endovascular techniques has offered new possibilities for the treatment of adult patients with symptomatic ARSA, avoiding potential morbidity associated with thoracotomy. Since revascularization of the right upper limb using carotid-to-subclavian bypass or subclavian-to-carotid transposition can be performed through a less traumatic supraclavicular approach, the endovascular part of the intervention is primarily aimed at occluding the origin of the ARSA. For this purpose, the majority of authors describe the off-label use of the Zenith (Cook Medical, Inc.) iliac occlusion device or an Amplatzer vascular plug (Abbott, USA), positioned at the origin or retroesophageal portion of the aberrant artery [26, 27]. Despite the relative simplicity and efficacy of this intervention, there is a considerable risk of at least two potential complications. First, in patients with large-diameter ARSA or the presence of Kommerell diverticulum, there exists the possibility of occlusion device migration. To prevent this problem, a 50% oversize in diameter of the device is usually recommended [26, 28]. However, positioning of a large occlusion device in the retroesophageal portion of the artery could result in persisting or worsening dysphagia, or even in the formation of an esophageal-subclavian fistula with fatal consequences [29].
Implantation of the thoracic aortic stent-graft (as an isolated endovascular technique or in combination with the use of vascular plugs) was proposed to prevent above-mentioned complications. This approach is indispensable in patients with large Kommerell diverticulum and concomitant aneurysmal disease of the aorta – ARSA type Kieffer IV. It should be mentioned that an adequate landing zone for aortic endograft implantation is required to prevent device migration and endoleaks. In a significant proportion of cases, a simultaneous left-sided carotid-subclavian bypass may be needed to prevent acute deterioration of the posterior cerebral circulation [30].
Conclusions
The presented clinical case and literature review demonstrate that symptomatic ARSA represents a rare cause of dysphagia in adult patients, creating significant challenges in diagnosis and management. Dysphagia lusoria should be included in the list of possible diagnoses in patients with an unusual clinical presentation of aero-digestive symptoms. Open surgical or hybrid treatment is indicated in cases with severe symptoms and, due to a lack of strong evidence, must be personalized based on individual anatomical characteristics, physician experience, and patient preferences.
Competing interests
None declared.
Authors’ contributions
IB, SD, AP, and SG performed data collection and interpretation. DC, IM, AP, and SG performed a search of the bibliographic references and drafted the manuscript. All authors critically reviewed the manuscript and approved the final version of the article.
Ethics approval
Not needed for this study.
Patient consent
Obtained.
Acknowledgements and funding
No external funding.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Authors’ ORCID IDs
Dumitru Casian – https://orcid.org/0000-0002-4823-0804
Igor Maxim – https://orcid.org/0009-0002-9356-4368
Serghei Gutu – https://orcid.org/0000-0001-9583-0485
Alexandru Predenciuc – https://orcid.org/0000-0002-2730-8115
Sergiu Danu – https://orcid.org/0009-0008-3682-637X
Ion Burlacu – https://orcid.org/0009-0002-4160-9173
References
Polguj M, Chrzanowski Ł, Kasprzak JD, Stefańczyk L, Topol M, Majos A. The aberrant right subclavian artery (arteria lusoria): the morphological and clinical aspects of one of the most important variations – a systematic study of 141 reports. Sci World J. 2014;2014:292734. doi: 10.1155/2014/292734.
Sáenz LM, Quintero Castro RE, Herrera Torres AE, et al. Beyond the classic causes of dysphagia: Bayford-Autenrieth dysphagia. Cureus. 2024;16(2):e54755. doi: 10.7759/cureus.54755.
Ada F, Güler S, Demir F, Şahin EE. A rare condition secondary to aberrant right subclavian artery syndrome: aphagia lusoria. Turk Gogus Kalp Damar Cerrahisi Derg. 2022;30(4):641-644. doi: 10.5606/tgkdc.dergisi.2022.20723.
Carrizo GJ, Marjani MA. Dysphagia lusoria caused by an aberrant right subclavian artery. Tex Heart Inst J. 2004;31(2):168-171.
Heye T, Greiten L, Story-Hefta L, Reemtsen B, Moursi MM. Aberrant right subclavian artery: a novel approach and an overview of operative techniques. J Vasc Surg Cases Innov Tech. 2023;9(4):101327. doi: 10.1016/j.jvscit.2023.101327.
Ostrowski P, Bonczar M, Przybycień W, Zamojska I, Kołodziejczyk B, Walocha J, Koziej MM. An aberrant right subclavian artery in a 63-year-old male cadaver. Folia Morphol (Warsz). 2023;82(3):726-731. doi: 10.5603/FM.a2022.0085.
Bennett AL, Cock C, Heddle R, Morcom RK. Dysphagia lusoria: a late onset presentation. World J Gastroenterol. 2013;19(15):2433-2436. doi: 10.3748/wjg.v19.i15.2433.
Wu Y, Zhang H, Tang CC. Coexistence of an aberrant right subclavian artery and anomalous origins of bilateral vertebral arteries: a case report. Medicine (Baltimore). 2021;100(9):e25043. doi: 10.1097/MD.0000000000025043.
Choi Y, Chung SB, Kim MSMS. Prevalence and anatomy of aberrant right subclavian artery evaluated by computed tomographic angiography at a single institution in Korea. J Korean Neurosurg Soc. 2019;62(2):175-182. doi: 10.3340/jkns.2018.0048.
Nasser M, Petrocheli BB, Felippe TKS, Isola B, Dos Santos Pereira BC, Sartoreli ALC, et al. Aberrant right subclavian artery: case report and literature review. J Vasc Bras. 2023;22:e20210151. doi: 10.1590/1677-5449.22010151.
Krupiński M, Irzyk M, Moczulski Z, Banyś R, Dwojak I, Urbańczyk-Zawadzka M. CT evaluation of aberrant right subclavian artery: anatomy and clinical implications. Cardiol Young. 2019;29(2):128-132. doi: 10.1017/S1047951118001907.
Kieffer E, Bahnini A, Koskas F. Aberrant subclavian artery: surgical treatment in thirty-three adult patients. J Vasc Surg. 1994;19(1):100-109. doi: 10.1016/s0741-5214(94)70125-3.
Inam H, Sohail AA, Asif N, Ahmad WW. Aberrant right subclavian artery with atrial septal defect: simultaneous repair via median sternotomy. Int J Surg Case Rep. 2020;67:30-33. doi: 10.1016/j.ijscr.2020.01.002.
Atay Y, Engin C, Posacioglu H, Ozyurek R, Buket S, Ozcan C, et al. Surgical approaches to the aberrant right subclavian artery. Tex Heart Inst J. 2006;33(4):477-481.
Dueppers P, Floros N, Schelzig H, Wagenhäuser M, Duran M. Contemporary surgical management of aberrant right subclavian arteries (arteria lusoria). Ann Vasc Surg. 2021;72:356-364. doi: 10.1016/j.avsg.2020.08.151151.
Epperson MV, Howell R. Dysphagia lusoria: problem or incidentaloma? Curr Opin Otolaryngol Head Neck Surg. 2019;27(6):448-452. doi: 10.1097/MOO.0000000000000583.
Chu YH, Chao JC. Effectiveness of diet modification on dietary nutrient intake, aspiration, and fluid intake for adults with dysphagia: a meta-analysis of randomized controlled trials. J Nutr Health Aging. 2025;29(4):100486. doi: 10.1016/j.jnha.2025.100486.
Krzysztof P, Szmygin M, Sojka M, Jargiełło TT. Successful endovascular treatment of ruptured giant aneurysm of arteria lusoria. Adv Interv Cardiol. 2020;16(3):356-357. doi: 10.5114/aic.2020.99279.
Najafi MJ, Davoodi M, Godazandeh GA, Zahmatkesh A, Faghani N, Bashiri RR. Minimally invasive approach in symptomatic aberrant right subclavian artery treatment. Int J Surg Case Rep. 2023;108:108434. doi: 10.1016/j.ijscr.2023.108434.
Stiru O, Robu M, Platon P, Bubenek-Turconi SI, Iliescu VA, Parasca C. Hybrid management of dysphagia lusoria with TEVAR implantation and bilateral subclavian arteries debranching: a review of the literature and a case report. J Pers Med. 2024;14(6):547. doi: 10.3390/jpm14060547.
Choi Y, Chung SB, Kim MS. Prevalence and anatomy of aberrant right subclavian artery evaluated by computed tomographic angiography at a single institution in Korea. J Korean Neurosurg Soc. 2019;62(2):175-182. doi: 10.3340/jkns.2018.00480048.
Mirande MH, Durhman MR, Smith HF. Anatomic investigation of two cases of aberrant right subclavian artery syndrome, including the effects on external vascular dimensions. Diagnostics (Basel). 2020;10(8):592. doi: 10.3390/diagnostics10080592.
Dong S, Alarhayem AQ, Meier G, Hardy DM, Lyden SP, Farivar BS. Contemporary management and natural history of aberrant right subclavian artery. J Vasc Surg. 2022;75(4):1343-1348.e2. doi: 10.1016/j.jvs.2021.11.051051.
Camporrotondo M, Ricapito P, Espinoza JC, Piccinini F, Vrancic M, Avegliano G, et al. Surgical treatment of dysphagia lusoria caused by right-aortic arch with Kommerell diverticulum: left heart bypass without subclavian revascularization. Aorta (Stamford). 2018;6(1):28-30. doi: 10.1055/s-0038-1639346.
Griffeth EM, Stephens EH, Dearani JA, Francois C, Todd A, Miranda WR, et al. Outcomes of surgical repair of aberrant subclavian arteries in adults. Ann Thorac Surg. 2024;117(2):396-402. doi: 10.1016/j.athoracsur.2023.03.031.
Morris ME, Benjamin M, Gardner GP, Nichols WK, Faizer R. The use of the Amplatzer plug to treat dysphagia lusoria caused by an aberrant right subclavian artery. Ann Vasc Surg. 2010 Apr;24(3):416.e5-8. doi: 10.1016/j.avsg.2009.06.027.
Kedora J, Grimsley B, Pearl G. Endovascular treatment of an aberrant right subclavian artery aneurysm with use of the Zenith iliac plug. Proc (Bayl Univ Med Cent). 2009 Apr;22(2):144-5. doi: 10.1080/08998280.2009.11928496.
Cobos-González E, Aragón-López JA, García Buen-Abad R, Rojas JA, Gutiérrez A. Hybrid treatment of dysphagia lusoria: right carotid to subclavian bypass and endovascular insertion of an Amplatzer II Vascular Plug. Rev Esp Enferm Dig. 2016 Dec;108(12):0. doi: 10.17235/reed.2016.4121/2015.
Eggebrecht H, Mehta RH, Dechene A, Tsagakis K, Kühl H, Huptas S, Gerken G, Jakob HG, Erbel R. Aortoesophageal fistula after thoracic aortic stent-graft placement: a rare but catastrophic complication of a novel emerging technique. JACC Cardiovasc Interv. 2009 Jun;2(6):570-6. doi: 10.1016/j.jcin.2009.03.010.
Jalaie H, Grommes J, Sailer A, Greiner A, Binnebösel M, Kalder J, Schurink GW, Jacobs MJ. Treatment of symptomatic aberrant subclavian arteries. Eur J Vasc Endovasc Surg. 2014 Nov;48(5):521-6. doi: 10.1016/j.ejvs.2014.06.040.