

Introduction
Psoriasis is a chronic inflammatory disease with a global prevalence ranging between 0.5% and 11.4% [1], characterized by T-cell dysfunction and persistent release of proinflammatory cytokines [2]. Beyond cutaneous and joint manifestations, the disease is associated with systemic comorbidities such as metabolic and cardiovascular disorders, and a moderately increased risk of lymphoproliferative malignancies, particularly lymphomas [3].
The etiology of non-Hodgkin lymphomas (NHL) remains incompletely understood. However, both severe immunosuppression and chronic immune stimulation are recognized as key risk factors. Immune homeostasis imbalance and chronic inflammation, together with immunosuppressive treatments (methotrexate, cyclosporine, anti-TNF agents), appear to contribute to lymphoma development in patients with psoriasis, especially in moderate-to-severe forms [3, 4].
A comprehensive 2020 meta-analysis including over 2 million patients reported a relative risk of 1.56 for lymphomas in general [5], while a 2024 North American study demonstrated a 1.5–1.8-fold increase in NHL risk in patients with mild to severe psoriasis [6].
Recent clinical case reports have also shown potential associations: Alali et al. (2021) described a case of Hodgkin’s lymphoma in a patient with psoriasis vulgaris under immunosuppressive therapy [7], and Scott et al. (2023) reported psoriasis–CTCL coexistence in 5.2% of analyzed cases [8]. Nevertheless, B-cell NHLs with cranial soft tissue localization and bone invasion remain exceptional.
In this context, we present a rare case of B-cell NHL with cranial involvement and bone extension in a patient with psoriasis vulgaris and an oncologic history. Its documentation offers valuable insights into the role of chronic inflammation in lymphoproliferative disorders and underlines the importance of an interdisciplinary clinical approach.
Case presentation
A 63-year-old male patient with a history of plaque-type psoriasis vulgaris and previous oncologic pathology (Clear cell renal carcinoma, T1N0M0, treated in 2021) presented for evaluation of a progressively enlarging, painless right temporo-parietal swelling, which had evolved over several months.
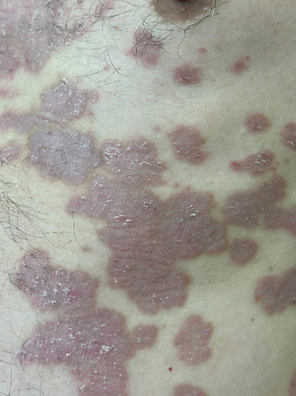
His psoriasis began in adulthood, around the age of 40, and followed a chronic, therapy-refractory course, with no complete remissions reported. Initial management included topical corticosteroids, but persistent lesions led to the initiation of systemic therapy with methotrexate. On dermatologic examination, the patient displayed extensive erythematous plaques with adherent white scaling and well-defined borders, located predominantly on the trunk, flanks, and lower limbs. Some lesions were confluent and lichenified, reflecting long-standing inflammation and insufficient treatment response (Figure 1a–d). Although the patient reported intermittent joint pain, standard radiographs revealed no significant articular changes suggestive of psoriatic arthritis.
 a |  b |
c |  d |
Figure 1a–d. Clinical appearance of chronic plaque-type psoriasis in a 63-year-old male patient. Multiple erythematous plaques with well-demarcated borders and thick, adherent silvery-white scales are observed on the anterior trunk (a, c), extensively on the lower limb (b), and left flank (d). Some lesions are confluent and show signs of chronicity, including lichenification and post-inflammatory hyperpigmentation. The patient reported persistent lesions despite topical corticosteroids and systemic methotrexate therapy. | |

In February 2021, a left renal tumor was surgically treated and histologically confirmed as clear cell carcinoma. In March 2021, the patient noted a painless subcutaneous nodular lesion in the right temporo-parietal area, initially interpreted as inflammatory or rheumatologic in origin, and received symptomatic treatment. Associated general symptoms included asthenia and xerostomia. In March 2022, cerebral MRI revealed a tumor in the right temporal soft tissues (48×19×50 mm), anterosuperior to the parotid gland, showing a gadolinium-enhancing lesion (~37 mm) in the parasagittal frontal bone on the right – suspicious for secondary bone invasion.
In April 2022, a biopsy of the tumor fragment was performed. Hematoxylin–eosin staining revealed a diffuse malignant lymphoid proliferation with areas of crush artifact. Immunohistochemical (IHC) analysis demonstrated diffuse positivity for CD20 and CD79a, consistent with mature B-cell phenotype, while CD45 confirmed lymphoid origin. CD3 expression was restricted to scattered reactive T-cells. The neoplastic cells were negative for BCL6, pancytokeratin (pCK), CD15, CD30, and CD68, findings that excluded a germinal-center phenotype, epithelial origin, classical Hodgkin lymphoma, or a histiocytic process. The overall immunophenotype supported the diagnosis of B-cell NHL NOS (WHO/ICD-O code 9590/3) .The disease was staged as IVA, with bone involvement and enlarged parotid lymph nodes on the right side.
Induction immunochemotherapy was initiated with 8 cycles of R-CHOP, consisting of rituximab, cyclophosphamide, doxorubicin hydrochloride, vincristine sulfate, and prednisone. PET/CT evaluation in June 2023 revealed a Deauville score of 3, indicating a partial favorable response. The patient was transitioned to maintenance biological therapy with rituximab monotherapy every 2 months, which was well tolerated and led to overall clinical improvement.
Discussion
B-cell NHL is a heterogeneous lymphoproliferative neoplasm with variable clinical presentations, ranging from indolent forms to aggressive variants with rapid systemic progression. It most commonly presents with peripheral lymphadenopathy and constitutional symptoms, while primary involvement of the soft tissues of the head with bone invasion is rarely documented in the literature [9]. In our case, the initial presentation was a subcutaneous, painless, slowly progressive right temporo-parietal mass, later confirmed by imaging and histology as aggressive B-cell lymphoma NOS with frontal bone invasion.
In the present case, the diagnostic process was particularly challenging due to the patient’s complex clinical background. The history of clear cell renal carcinoma raised an initial concern for metastatic disease, especially given the osteotropic behavior of renal cell carcinoma. However, the immunophenotype and the absence of epithelial or histiocytic markers effectively excluded this possibility. Cutaneous T-cell lymphoma was also considered, particularly in the context of psoriasis vulgaris, which can mask or mimic early CTCL. CD3 positivity restricted to reactive T-cells and the absence of T-cell lineage markers ruled out CTCL. The lack of BCL6 expression further argued against a germinal-center B-cell phenotype and supported the NOS classification.
The differential diagnosis included: bone metastasis from clear cell renal carcinoma (diagnosed in 2021), which was not supported by the immunophenotype; cutaneous T-cell lymphoma (CTCL), particularly in the context of underlying psoriasis vulgaris, as early CTCL can be clinically and histologically misdiagnosed as psoriasis [8]; and chronic inflammatory or granulomatous pseudotumoral lesions, which were excluded morphologically and immunohistochemically.
Psoriasis vulgaris represents an additional layer of complexity. Chronic immune activation, persistent systemic inflammation, and long-standing T-cell dysregulation have been associated with a moderately increased risk of lymphoproliferative disorders. Recent meta-analyses and cohort studies report a relative risk of 1.5–1.8 for lymphoma in patients with mild to severe psoriasis [4–6]. Although most associations involve Hodgkin lymphoma or CTCL, B-cell lymphomas have also been documented, suggesting a broader impact of chronic immune stimulation on lymphomagenesis. This case underscores the need for diagnostic vigilance when evaluating new or atypical masses in patients with chronic inflammatory dermatoses. Early biopsy and multidisciplinary evaluation—including dermatology, oncology, hematology, and radiology—are essential to avoid diagnostic delay in complex cases such as this.
Conclusions
This case highlights a rare presentation of aggressive B-cell NHL NOS with cranial soft-tissue involvement and bone erosion, posing significant diagnostic challenges given the patient’s long-standing psoriasis and prior oncologic history. Histopathology and immunohistochemistry were essential in distinguishing lymphoma from potential mimickers, including renal cell carcinoma metastasis and cutaneous T-cell lymphoma. The association with chronic psoriasis underscores the importance of considering lymphoproliferative disease in patients with persistent inflammatory dermatoses or atypical cutaneous lesions. This report reinforces the need for multidisciplinary evaluation and timely biopsy in order to avoid diagnostic delay in similar complex clinical settings.
Competing interests
None declared.
Authors’ contributions
MR conceived the study, participated in the clinical assessment and drafted the manuscript. MB contributed to dermatological evaluation and clinical monitoring of the patient. SB and PV were responsible for oncologic and hematologic management, including therapeutic decision-making and follow-up. DV performed the immunohistochemical analysis and interpretation. LS contributed to histopathological examination and diagnostic validation. All authors critically reviewed and approved the final version of the manuscript.
Acknowledgements and funding
This study did not receive any external funding. The authors would like to thank the medical team involved in the patient's care at the Oncology Institute and the Department of Dermatology for their interdisciplinary collaboration.
Informed consent for publication
Obtained.
Ethics approval
Not needed for this article.
Provenance and peer review
Not commissioned, externally peer review.
Authors’ ORCID IDs
Mihaela Rotari – https://orcid.org/0009-0002-6833-1845
Mircea Bețiu – https://orcid.org/0000-0003-0824-3480
Sanda Buruiană – https://orcid.org/0000-0003-2341-0099
Valeria Pînzaru – https://orcid.org/0009-0000-8834-7743
Valeriu David – https://orcid.org/0000-0001-9799-7369
Lilian Șaptefrați – https://orcid.org/0000-0003-2779-718X
References
Ngan V. Guidelines for the management of psoriasis. In: DermNet® [Internet]. Auckland: DermNet; 2023 [cited 2025 Jul 21]. Available from: https://dermnetnz.org/topics/guidelines-for-the-treatment-of-psoriasis
Zhang P, Su Y, Li S, Chen H, Wu R, Wu H. The roles of T cells in psoriasis. Front Immunol. 2023;14:1081256. doi: 10.3389/fimmu.2023.1081256.
Takeshita J, Grewal S, Langan SM, et al. Psoriasis and comorbid diseases: epidemiology. J Am Acad Dermatol. 2017;76(3):377-390. doi: 10.1016/j.jaad.2016.07.064.
Patel RV, Clark LN, Lebwohl M, Weinberg JM. Treatments for psoriasis and the risk of malignancy. J Am Acad Dermatol. 2009 Jun;60(6):1001-1017. doi: 10.1016/j.jaad.2008.12.031.
Vaengebjerg S, Skov L, Egeberg A, Loft ND. Prevalence, incidence, and risk of cancer in patients with psoriasis and psoriatic arthritis: a systematic review and meta‑analysis. JAMA Dermatol. 2020;156(4):421-429. doi: 10.1001/jamadermatol.2020.0024.
Diaz MJ, Haq Z, Tran JT, Abdi P, Motaparthi K, Grant‑Kels JM, Montanez‑Wiscovich ME. Psoriasis and non‑Hodgkin’s lymphoma in a diverse sample of U.S. adults: a propensity matched case‑control study. J Am Acad Dermatol. 2024 Jul;91(1):104-107. doi: 10.1016/j.jaad.2024.02.040.
Alali Z, Al Ashour BH, Alrefaee M. Hodgkin's lymphoma in the context of psoriasis vulgaris treated with immunosuppressive therapy: a case report and review of literature. Cureus. 2021;13(11):e19490. doi: 10.7759/cureus.19490.
Scott J, Lai C, Coltart G, et al. Coexistence of psoriasis and cutaneous T-cell lymphoma. Clin Exp Dermatol. 2023;48(10):1155-1159. doi: 10.1093/ced/llad213.
Rezaei‑Kalantari K, Samimi K, Jafari M, Karimi MA, Ansari K, Davoodi M, et al. Primary diffuse large B‑cell lymphoma of the cranial vault. Iran J Radiol. 2012;9(2):88-92. doi: 10.5812/iranjradiol.7734.
Rule S, Barreto WG, Briones J, Carella AM, Casasnovas O, Pocock C, et al. Efficacy and safety assessment of prolonged maintenance with subcutaneous rituximab in patients with relapsed or refractory indolent non-Hodgkin lymphoma: results of the phase III MabCute study. Haematologica. 2022;107(2):500-509. doi: 10.3324/haematol.2020.274803.