
Introduction
The efficiency of orthodontic therapy is largely dependent on the mechanical response and biomechanical properties of the archwires used during treatment [1, 2]. The evolution of orthodontic techniques over the past decades has been strongly influenced by the search for optimal force systems capable of achieving precise tooth movement in a shorter time and with improved patient comfort [3, 4]. Traditional wire progressions, such as those proposed by Tweed (1946) and Ricketts (1982), rely on a sequence of archwires with progressively increasing rigidity and dimensions [5, 6]. Although this conventional approach ensures controlled movement and stability, it often requires an extended treatment duration due to multiple wire changes and the biological adaptation time of the periodontal structures [7].
In contrast, modern orthodontics has shifted towards the development of low-friction systems and wide archwire designs, which aim to simplify mechanics and reduce treatment time. Damon (2004) and McLaughlin (2011) have introduced self-ligating brackets and preformed wide arch forms that promote more physiological expansion of the dental arches and better accommodation of the tongue space [8, 9]. These innovations are claimed to minimize the need for extractions, improve facial aesthetics, and enhance stability by promoting a more balanced arch form [10-12].
However, despite the widespread clinical adoption of wide and extra-wide archwire systems, there remains a need for objective and quantitative evidence to support their claimed advantages over standard archwire forms. The biomechanical effects, degree of arch expansion, and overall treatment efficiency achieved through such systems remain only partially understood and variably reported in the literature [13-15]. Factors such as initial malocclusion type, periodontal condition, and patient-specific anatomical variations can significantly influence treatment outcomes [16].
Therefore, the present study aims to evaluate the efficiency of orthodontic expansion methods using wide and extra-wide archwires in the treatment of dentoalveolar malocclusions. By comparing these modern systems with conventional archwire progressions, this research seeks to provide clinically relevant data on treatment duration, degree of transverse expansion, and stability of achieved results [17-19]. The outcomes will contribute to the orthodontic research community by validating – or potentially refuting – the claims made regarding the superiority of wide and extra-wide archwire systems in enhancing treatment efficiency and biomechanical harmony [20, 21].
Materials and methods
Study design. This observational cohort study was carried out between 2020 and 2025 at the Ilarion Postolachi Department of Orthopedic Stomatology, Nicolae Testemițanu State University of Medicine and Pharmacy, Chișinău, Republic of Moldova, and the Galadent Prim Clinic. The research protocol was reviewed and approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (Minutes No. 47/2020, dated March 15, 2020). Written informed consent was obtained from all participants prior to their inclusion in the study. Patients in the control group (n=100) were treated using the conventional fixed appliance protocol with standard NiTi/SS archwire sequences, whereas subjects in the alternative group (n=80) underwent orthodontic treatment employing wide and extra-wide CuNiTi/TA/TMA/SS archwires.
The study inclusion criteria comprised patients presenting dentomaxillary anomalies associated with dental space deficiency. Exclusion criteria included a history of previous orthodontic or maxillofacial treatment, congenital craniofacial malformations, and facial asymmetries requiring surgical management. Diagnostic assessment was based on comprehensive clinical and photographic examination, digital biometric analysis using Medit Link and NemoCast software, as well as radiographic evaluation performed according to the Tweed, Ricketts, and Roth-Jarabak cephalometric methods. [22].
Treatment Protocol: All patients were treated with a standard fixed multibracket appliance (0.022-inch slot), following a sequential archwire system using NiTi, CuNiTi, and TMA wires [23].
- Stage 1: Initial alignment and leveling – superelastic NiTi archwires (0.012–0.014 inch) (Fig. 1)
- Stage 2: Controlled transverse expansion – CuNiTi archwires (0.016 × 0.022 inch and 0.017 × 0.025 inch) (Fig. 2)
- Stage 3: Finishing and consolidation – TMA archwires (0.019 × 0.025 inch) (Fig. 3, 4)
 |  |
Fig. 1 Schematic representation of transverse dentoalveolar expansion with a CuNiTi archwire (active phase). | Fig. 2 Controlled transverse expiation using CuNiTi archwires (0.016 × 0.022 inch and 0.017 × 0.025 inch): schematic representation of lateral expansion forces. |
 | 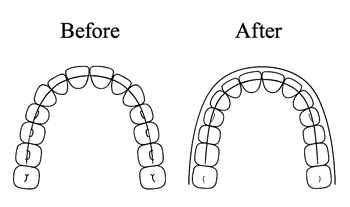 |
Fig. 3 Finishing and consolidation – TMA archwires (0.019 × 0.025 inch). | Fig. 4 Before and after finishing. |
Statistical analysis was performed using the RStudio open-source software. The mean with a 95% confidence interval, median, standard deviation, interquartile range, and minimal and maximal values were considered for descriptive statistics of numerical variables. For categorical parameters, absolute and relative frequencies with a 95% confidence interval were estimated. Comparative evaluation between the groups was performed using the Mann-Whitney test (visualization through boxplots and jitter plots), completed by a rank biserial correlation analysis (rrb) for practical significance estimation in numerical variables. Pearson’s Chi-squared test with Monte Carlo simulation was applied for association hypothesis testing for categorical variables.
Results
The study included a total of 180 participants, divided into the Alternative group (n = 80) and the Classic group (n = 100). The overall mean age was 18.6 ± 5.1 years, with no statistically significant age difference between the two treatment groups (p = 0.20). Age distribution was comparable between groups, with similar medians and interquartile ranges.
A statistically significant difference was observed in gender distribution between the two groups (χ² = 5.2, p = 0.032). Females predominated in the overall sample (71.1%), with a higher proportion in the Classic group (78.0%) compared to the Alternative group (62.5%). No significant differences were found regarding settlement (urban vs. rural) between groups (p = 0.10).
The distribution of constitutional craniofacial types (brachyfacial, dolichocephalic, and mesocephalic) was similar between groups, with the brachyfacial type being the most prevalent (approximately 59%), and no statistically significant differences were detected (p > 0.9).
Regarding Angle’s classification, Class I malocclusion was the most common in the overall sample (60.6%). Although a higher proportion of Class I was observed in the Alternative group and a higher proportion of Class II in the Classic group, these differences were not statistically significant (p = 0.069).
Analysis of occlusal relationships revealed no statistically significant differences between groups for: RMR (Right Molar Relationship) (p > 0.9), RML (Left Molar Relationship) (p = 0.50), RCR (Right Canine Relationship) (p = 0.40), and RCL (Left Canine Relationship) (p = 0.30).
Across all participants, Class I molar and canine relationships were the most prevalent on both sides, followed by Class II, while Class III relationships were relatively rare.
Overall, aside from gender distribution, the Alternative and Classic groups were comparable with respect to demographic characteristics, craniofacial morphology, Angle classification, and molar and canine sagittal relationships, indicating good baseline homogeneity between groups (Table 1).
Transverse expansion outcomes. The analysis of transverse maxillary dimensions (Table 2) demonstrated a high degree of similarity between the Alternative and Classic groups at both the initial and final evaluations. At baseline, the initial intercanine width (DMSICT) showed comparable mean values and distributions in the two groups, indicating similar transverse maxillary morphology in the anterior region. Likewise, the initial inter-first premolar (DMSIPIT), inter-second premolar (DMSIPIIT), and intermolar widths (DMSIMT) did not differ significantly between groups (all p > 0.05).
At the anterior maxillary level, the intercanine transverse dimension (DMSICT) showed identical mean values in both groups (34.0 ± 3.0 mm in the Alternative group and 34.0 ± 2.9 mm in the Classic group), with similar median values (34 mm) and overlapping ranges (27.0–41.0 mm and 28.0–40.0 mm, respectively). Likewise, the first premolar transverse width (DMSFCT) demonstrated comparable mean values between the Alternative group (35.8 ± 2.8 mm) and the Classic group (36.0 ± 2.6 mm), with overlapping confidence intervals and no statistically significant difference (p = 0.7). Measurements at the premolar and intermediate regions further confirmed this pattern. The DMSIPIT parameter showed almost identical mean values in the Alternative and Classic groups (36.1 ± 3.2 mm vs. 36.0 ± 2.8 mm), while the DMSFPIT parameter recorded mean transverse widths of 39.0 ± 2.9 mm and 39.0 ± 3.1 mm, respectively. For both variables, medians and interquartile ranges were highly similar, and statistical testing revealed no significant intergroup differences (p > 0.8). At the intermediate posterior level, DMSIPIIT and DMSFPIIT measurements remained consistent between groups, with mean values ranging from 40.7 to 40.9 mm and from 43.7 to 43.8 mm, respectively. The confidence intervals overlapped extensively, and no statistically significant differences were detected (p > 0.9). In the posterior maxillary region, intermolar transverse dimensions (DMSIMT and DMSFMT) were also comparable. Mean DMSIMT values were 49.1 ± 4.1 mm in the Alternative group and 49.8 ± 3.7 mm in the Classic group, while DMSFMT values were identical in both groups (51.8 ± 3.8 mm). The Wilcoxon rank-sum test confirmed the absence of statistically significant differences between groups for these parameters (p = 0.2 and p = 0.8, respectively).
Overall, the absence of statistically significant differences across all transverse maxillary measurements indicates that the Alternative and Classic groups were homogeneous with respect to transverse maxillary morphology. This homogeneity supports the validity of intergroup comparisons and suggests that observed outcomes are unlikely to be influenced by baseline transverse maxillary discrepancies.
Table 1. Demographic and Clinical Characteristics of the Study Populations | ||||||||
|---|---|---|---|---|---|---|---|---|
Group | Overall N = 1801 | 95% CI2 | Alternative N = 801 | 95% CI2 | Classic N = 1001 | 95% CI2 | Statistic Test3 | p-value3 |
Age | 18.6 (5.1) 17.0 (6.0) 14.0 36.0 | 18, 19 | 18.5 (5.5) 16.0 (7.0) 14.0 36.0 | 17, 20 | 18.8 (4.8) 17.0 (6.3) 14.0 36.0 | 18, 20 | 3,583 | 0.2 |
Gender |
|
|
|
|
|
| 5.2 | 0.032 |
F | 128 (71.1%) | 64%, 78% | 50 (62.5%) | 52%, 73% | 78 (78.0%) | 70%, 86% |
|
|
M | 52 (28.9%) | 22%, 36% | 30 (37.5%) | 27%, 48% | 22 (22.0%) | 14%, 30% |
|
|
Settlement |
|
|
|
|
|
| 3.0 | 0.10 |
Town | 94 (52.2%) | 45%, 60% | 36 (45.0%) | 34%, 56% | 58 (58.0%) | 48%, 68% |
|
|
Village | 86 (47.8%) | 40%, 55% | 44 (55.0%) | 44%, 66% | 42 (42.0%) | 32%, 52% |
|
|
Constitutional type |
|
|
|
|
|
| 0.17 | >0.9 |
Brachyfacial | 106 (58.9%) | 52%, 66% | 47 (58.8%) | 48%, 70% | 59 (59.0%) | 49%, 69% |
|
|
Dolichocephalic | 52 (28.9%) | 22%, 36% | 24 (30.0%) | 20%, 40% | 28 (28.0%) | 19%, 37% |
|
|
Mesocephalic | 22 (12.2%) | 7.4%, 17% | 9 (11.3%) | 4.3%, 18% | 13 (13.0%) | 6.4%, 20% |
|
|
Angle |
|
|
|
|
|
| 5.4 | 0.069 |
cl. I | 109 (60.6%) | 53%, 68% | 56 (70.0%) | 60%, 80% | 53 (53.0%) | 43%, 63% |
|
|
cl. II | 53 (29.4%) | 23%, 36% | 18 (22.5%) | 13%, 32% | 35 (35.0%) | 26%, 44% |
|
|
cl. III | 18 (10.0%) | 5.6%, 14% | 6 (7.5%) | 1.7%, 13% | 12 (12.0%) | 5.6%, 18% |
|
|
RMR |
|
|
|
|
|
| 0.04 | >0.9 |
cl. I | 102 (56.7%) | 49%, 64% | 46 (57.5%) | 47%, 68% | 56 (56.0%) | 46%, 66% |
|
|
cl. II | 62 (34.4%) | 28%, 41% | 27 (33.8%) | 23%, 44% | 35 (35.0%) | 26%, 44% |
|
|
cl. III | 16 (8.9%) | 4.7%, 13% | 7 (8.8%) | 2.6%, 15% | 9 (9.0%) | 3.4%, 15% |
|
|
RML |
|
|
|
|
|
| 1.5 | 0.5 |
cl. I | 104 (57.8%) | 51%, 65% | 47 (58.8%) | 48%, 70% | 57 (57.0%) | 47%, 67% |
|
|
cl. II | 58 (32.2%) | 25%, 39% | 23 (28.8%) | 19%, 39% | 35 (35.0%) | 26%, 44% |
|
|
cl. III | 18 (10.0%) | 5.6%, 14% | 10 (12.5%) | 5.3%, 20% | 8 (8.0%) | 2.7%, 13% |
|
|
RCR |
|
|
|
|
|
| 2.2 | 0.4 |
cl. I | 76 (42.2%) | 35%, 49% | 29 (36.3%) | 26%, 47% | 47 (47.0%) | 37%, 57% |
|
|
cl. II | 97 (53.9%) | 47%, 61% | 48 (60.0%) | 49%, 71% | 49 (49.0%) | 39%, 59% |
|
|
cl. III | 7 (3.9%) | 1.1%, 6.7% | 3 (3.8%) | 0.00%, 7.9% | 4 (4.0%) | 0.16%, 7.8% |
|
|
RCL |
|
|
|
|
|
| 2.4 | 0.3 |
cl. I | 58 (32.2%) | 25%, 39% | 21 (26.3%) | 17%, 36% | 37 (37.0%) | 28%, 46% |
|
|
cl. II | 106 (58.9%) | 52%, 66% | 51 (63.8%) | 53%, 74% | 55 (55.0%) | 45%, 65% |
|
|
cl. III | 16 (8.9%) | 4.7%, 13% | 8 (10.0%) | 3.4%, 17% | 8 (8.0%) | 2.7%, 13% |
|
|
Note: 1Mean (SD), Median (IQR), Min Max; n (%), 2CI = Confidence Interval, 3Wilcoxon rank sum test; Pearson’s Chi-squared test with simulated p-value (based on 105 replicates) | ||||||||
Table 2. Maxillary Transverse Arch Measurement Data | ||||||||
Group | Overall N = 1801 | 95% CI2 | Alternative N = 801 | 95% CI2 | Classic N = 1001 | 95% CI2 | Statistic Test3 | p-value3 |
DMSICT | 34.0 (2.9) 34.0 (4.0) 27.0 41.0 | 34, 34 | 34.0 (3.0) 34.0 (4.0) 27.0 41.0 | 33, 35 | 34.0 (2.9) 34.0 (4.0) 28.0 40.0 | 33, 35 | 3,984 | >0.9 |
DMSFCT | 35.9 (2.7) 35.8 (2.6) 28.0 45.0 | 36, 36 | 35.8 (2.8) 35.5 (2.0) 28.0 43.0 | 35, 36 | 36.0 (2.6) 36.0 (3.0) 31.0 45.0 | 36, 37 | 3,886 | 0.7 |
DMSIPIT | 36.1 (3.0) 36.0 (4.0) 29.0 45.0 | 36, 36 | 36.1 (3.2) 36.0 (4.0) 29.0 45.0 | 35, 37 | 36.0 (2.8) 36.0 (3.3) 29.0 45.0 | 35, 37 | 4,049 | 0.9 |
DMSFPIT | 39.0 (3.0) 39.0 (4.0) 31.0 50.0 | 39, 39 | 39.0 (2.9) 39.0 (3.6) 33.0 49.0 | 38, 40 | 39.0 (3.1) 39.0 (4.0) 31.0 50.0 | 38, 40 | 3,921 | 0.8 |
DMSIPIIT | 40.8 (3.4) 41.0 (5.0) 31.0 50.0 | 40, 41 | 40.7 (3.6) 40.0 (5.0) 31.0 48.0 | 40, 42 | 40.9 (3.2) 41.0 (4.5) 33.0 50.0 | 40, 41 | 3,997 | >0.9 |
DMSFPIIT | 43.7 (3.1) 44.0 (3.5) 35.0 55.0 | 43, 44 | 43.8 (3.2) 44.0 (3.9) 37.5 55.0 | 43, 45 | 43.7 (3.1) 44.0 (3.0) 35.0 52.0 | 43, 44 | 4,040 | >0.9 |
DMSIMT | 49.5 (3.9) 50.0 (5.0) 40.5 60.0 | 49, 50 | 49.1 (4.1) 50.0 (5.0) 40.5 60.0 | 48, 50 | 49.8 (3.7) 50.0 (5.0) 41.0 59.0 | 49, 51 | 3,599 | 0.2 |
DMSFMT | 51.8 (3.8) 52.0 (5.0) 42.0 61.0 | 51, 52 | 51.8 (3.8) 52.0 (5.0) 42.0 59.0 | 51, 53 | 51.8 (3.8) 51.5 (5.0) 42.0 61.0 | 51, 53 | 4,100 | 0.8 |
Note: 1n (%); Mean (SD), Median (IQR), Min Max, 2CI = Confidence Interval, 3Wilcoxon rank sum test | ||||||||
Treatment duration. Treatment duration differed markedly between protocols. In the overall cohort, the mean duration was 25.0 ± 6.5 months (median 24.0 months; range 12–39 months). Patients treated with the Alternative method completed therapy in 20.2 ± 4.4 months (median 19.0 months; range 12–38 months), whereas those in the Classic group required 28.9 ± 5.2 months (median 30.0 months; range 14–39 months). This difference of 8.7 months was both statistically significant (p < 0.001) and clinically relevant. An inverse and strong correlation was observed between treatment duration and the magnitude of transverse expansion (r = –0.69), indicating that greater controlled widening of the dental arches was associated with shorter overall treatment time (Fig. 5). No increase in post-treatment relapse incidence was detected in the Alternative group, suggesting that the more rapid expansion did not compromise occlusal stability.
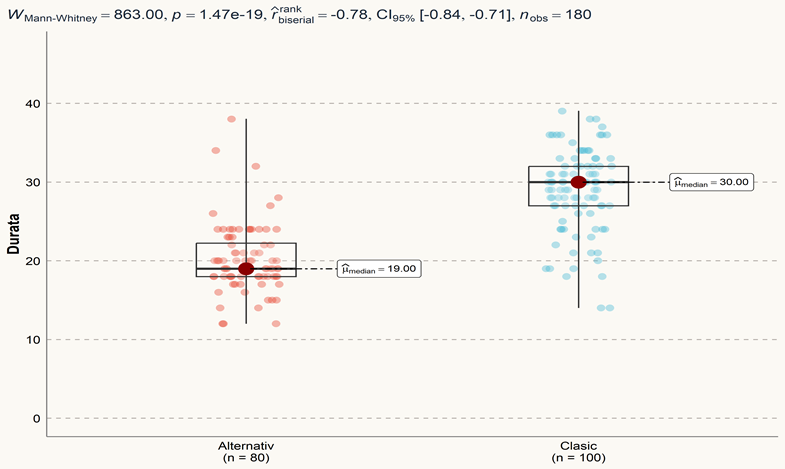 |
Fig. 5 Graphical representation of treatment duration (months) between the Alternative and Classic groups Note: Boxes represent the interquartile range (IQR), the horizontal line within each box indicates the median value, and whiskers denote the minimum and maximum recorded treatment durations. W represents the Mann–Whitney U test statistic; p denotes the probability value indicating statistical significance; rrb indicates the rank-biserial correlation coefficient (effect size); CI95% represents the 95% confidence interval of the effect size; and nobs denotes the total number of observations included in the analysis. |
Discussion
This study evaluated the efficiency of wide and extra-wide archwires in orthodontic expansion therapy and demonstrated that their use results in significantly greater transverse dentoalveolar widening and substantially shorter treatment durations compared with a conventional archwire protocol. Because the two groups were similar at baseline in terms of age, occlusal characteristics, and cephalometric parameters, the observed differences are most plausibly attributable to the archwire strategy rather than to sample imbalance. The transverse dimensions at the canine, premolar, and molar levels were comparable between the two groups under similar clinical conditions; however, the Alternative protocol achieved these equivalent transverse outcomes within a shorter overall treatment duration. These findings are consistent with previous reports that low-friction, wide-arch systems can enhance transverse development and reduce the need for extractions while preserving facial aesthetics and stability. The systematic increase in DMSICT/DMSFCT and DMSIPIT/DMSFPIT, along with the relatively narrow dispersion of post-treatment values, suggests that expansion was controlled rather than excessive. A major clinical implication of the present work is the significant reduction in treatment time – approximately 8–9 months shorter with the wide archwire protocol. This result is in line with studies reporting slight to moderate decreases in treatment duration when low-friction systems or expanded archforms are used. Importantly, in our sample, this acceleration did not appear to compromise post-treatment stability, as no increase in relapse incidence was observed in the Alternative group during the documented follow-up period. The nearly normal distributions of DMSIPIT and DMSFPIT further support the predictability of the biomechanical response. Mild outliers in the final measurements did not translate into clinical instability and may reflect individual anatomical variability. Recent three-dimensional studies emphasize the value of digital models for assessing arch form and symmetry, and similar approaches could be applied in future prospective trials to quantify volumetric changes and periodontal responses to wide archwire expansion. This study has limitations. Its retrospective design may introduce selection bias, and the significant difference in gender distribution between groups could serve as an uncontrolled confounder. In addition, although transverse and cephalometric measurements were detailed, skeletal maturation stages and long-term (>5 years) retention outcomes were not systematically evaluated. Future research should include prospective randomized trials using three-dimensional imaging, standardized retention protocols, and multivariate analysis to control simultaneously for demographic, skeletal, and occlusal variables. Despite these limitations, the present findings provide robust clinical evidence that wide and extra-wide archwires can be safely incorporated into contemporary orthodontic practice to improve efficiency. When carefully selected and monitored, such mechanics offer predictable transverse gains and meaningful reductions in treatment duration without compromising occlusal stability.
Conclusions
The Alternative protocol enhances treatment efficiency without compromising transverse outcomes or post-treatment stability, while wide archwire mechanics represent a reliable approach for managing dentoalveolar crowding in contemporary orthodontic practice; however, further prospective studies are required to confirm these findings.
Competing interests
None declared.
Authors’ contributions
MJV conceived and designed the study, collected the data, performed the analysis and interpretation of the data, drafted the manuscript, and takes responsibility for the integrity of the work as a whole. OS contributed to drafting the manuscript and critically reviewed it for important intellectual content. OA supervised the study process, contributed to the study design and methodology validation, performed the statistical analysis, and provided critical revision of the manuscript.
Ethics approval
The research project was approved by the Research Ethics Committee of the Nicolae Testemițanu State University of Medicine and Pharmacy (Minutes no. 47/2020 dated March 15, 2020).
Patient consent
Obtained.
Acknowledgements and funding
No external funding.
Provenance and peer review
Not commissioned, externally peer reviewed.
Authors’ ORCID IDs
Mihaela Jarovlea-Bejenari– https://orcid.org/0000-0001-9145-3192
Oleg Solomon –https://orcid.org/0000-0002-7341-1711
Oleg Arnaut – https://orcid.org/0000-0002-5483-8672
References
Burstone CJ. Biomechanics of deep overbite correction. Semin Orthod. 2001;7(1):26-33. doi: 10.1053/sodo.2001.21059.
Melsen B, editor. Adult orthodontics. Oxford: Wiley-Blackwell; 2012.
Graber LW, Vanarsdall RL Jr, Vig KWL, Huang GJ. Orthodontics: current principles and techniques. 6th ed. St. Louis: Elsevier; 2017. 1016 p.
Proffit WR, Fields HW, Larson BE, Sarver DM. Contemporary orthodontics. 6th ed. Philadelphia: Elsevier; 2019.729 p.
Ricketts RM. Bioprogressive therapy as an answer to orthodontic needs. Part I. Am J Orthod. 19976;70(3):241-268. doi: 10.1016/0002-9416(76)90332-8.
Tweed CH. The Frankfort-mandibular plane angle in orthodontic diagnosis, classification, treatment planning and prognosis. Am J Orthod. 1946;32(4):175-230. doi: 10.1016/0096-6347(46)90001-4.
Leon-Valencia J, Alarcon JA, Martin C. Assessment of dental arch width expansion effectiveness using a novel hybrid aligner with virtual brackets and nickel-titanium archwires: a prospective clinical study. Appl Sci. 2025;15(1):39. doi: 10.3390/app15010039.
Damon DH. The Damon low-friction bracket: a biologically compatible straight-wire system. J Clin Orthod. 1998;32(11):670-680.
McLaughlin RP, Bennett JC, Trevisi HJ. Systemized orthodontic treatment mechanics. Edinburgh: Mosby; 2001.324 p.
Nanda R. Biomechanics and esthetic strategies in clinical orthodontics. St. Louis: Elsevier Saunders; 2005. 385 p.
Pandis N, Miles PG. Treatment efficiency with self-ligating brackets: the clinical evidence. Semin Orthod. 2010;16(4):258-265. doi: 10.1053/j.sodo.2010.06.004.
Trifan V, Lupan I, Trifan D, Calfa S. Morbiditatea prin anomaliile dento-maxilare în Republica Moldova [Morbidity by dental-maxillary anomalies the Republic of Moldova]. Stomatol Med (Chisinau). 2015;(1):47-52. Romanian.
Dehbi H, Azaroual MF, Zaoui F, Halimi A, Benyahia H. Efficacité thérapeutique des brackets auto-ligaturants: revue systématique. Int Orthod. 2017;15(3):297-311. doi: 10.1016/j.ortho.2017.06.010.
Fleming PS, Johal A. Self-ligating brackets in orthodontics: a systematic review. Angle Orthod. 2010;80(3):575-584. doi: 10.2319/081009-454.1.
Tachi A, Tochigi K, Saze N, Arai K. Impact of the prefabricated forms of NiTi archwires on orthodontic forces delivered to the mandibular dental arch. Prog Orthod. 2021;22(1):41. doi: 10.1186/s40510-021-00385-1.
Allan D, Woods MG. Arch-dimensional changes in non-extraction cases with finishing wires of a particular material, size and arch form. Aust Orthod J. 2015;31(1):26-36.
Mahmood B, Hassan B. Three-dimensional analysis of dental arch form and dimensions in a sample of Kurdish students in Hawler Medical University. Erbil Dent J. 2023;6(1). doi: 10.15218/edj.2023.01.
Mateu ME, Benítez-Rogé S, Calabrese D, Lumi M, Iglesias M, Méndez P, et al. Prospective clinical study of transverse development with self-ligating brackets. Acta Odontol Latinoam. 2020;33(2):112-116.
Nguyen M, Al-Moghrabi D, Tomlinson L, Azami N, Dolce C, Abu Arqub S. Early orthodontic treatment practices and perceptions: a cross-sectional survey of AAO members. J Orthod. 2025;52(3):285-294. doi: 10.1177/14653125251358832.
Arora MA, Shah A, Somani D. Self-ligating versus conventional brackets: a narrative review. Cureus. 2025;17(3):e81499. doi: 10.7759/cureus.81499.
Serrano-Velasco D, Martín-Vacas A, Giovannini G, Paz-Cortés MM, Aragoneses JM. Accuracy analysis of digital models from intraoral scanners and 3D-printed casts in children and teenagers. Children (Basel). 2024;11(9):1082. doi: 10.3390/children11091082.
Andrews LF. The straight-wire appliance. Br J Orthod. 1979;6(3):125-143. doi: 10.1179/bjo.6.3.125.