

Introduction
Recurrent laryngeal papillomatosis is a benign condition affecting the mucosa of the respiratory tract, characterized by the repeated formation of exophytic lesions caused by infection with the human papillomavirus. Although often referred to as glottic or laryngeal papillomatosis, the disease can affect any part of the respiratory tract [1-3]. Despite being relatively rare, recurrent laryngeal papillomatosis’s tendency to recur and its impact on respiratory function pose a significant challenge for both patients and healthcare systems [4-6]. Males are more frequently affected than females [6, 7]. Clinical manifestations may resemble other common respiratory conditions, such as asthma or bronchitis, which can delay diagnosis and the initiation of appropriate treatment [7, 8]. In severe cases, airway obstruction may require urgent interventions, including tracheotomy, to ensure adequate breathing [9, 10].
The incidence of recurrent laryngeal papillomatosis varies significantly worldwide, influenced by factors such as human papillomavirus infection rates, access to medical care, and case reporting practices. In the pediatric population, the estimated incidence ranges from 0.2 to 2.1 cases per 100 thousand children annually, with reported prevalence between 0.8-4.3 per 100,000. The juvenile form is characterized by the recurrent appearance of exophytic lesions in the larynx, and disease severity can vary widely, often requiring frequent surgical interventions and adjuvant therapies [10-13].
A clear understanding of the epidemiological aspects of recurrent laryngeal papillomatosis is essential for developing effective strategies for the prevention, early detection, and management of this rare but impactful condition affecting children's health. In this context, the present chapter analyzes the demographic distribution of recurrent laryngeal papillomatosis in the Republic of Moldova, based on data collected over recent decades, highlighting trends in incidence and prevalence by age, sex, and time period. Special attention is given to identifying high-risk groups and the local particularities of disease progression [14, 15].
At the same time, the study evaluates the social and economic implications of the disease, taking into account the costs associated with repeated hospitalizations, surgical treatments, and the psychological impact on affected children and their families. The analysis is based exclusively on national statistical data, providing an updated and context-specific overview for the Republic of Moldova. This information may support the development of public health policies, the adjustment of human papillomavirus vaccination strategies, and the improvement of clinical management. By identifying region-specific needs, the study aims to support informed decision-making in the field of pediatric otorhinolaryngology.
Given the lack of consolidated epidemiological data on recurrent laryngeal papillomatosis in the pediatric population of the Republic of Moldova, this study aims to make a significant contribution to understanding the national distribution and progression of the disease. The statistical analysis of cases recorded over an extended period provides a solid foundation for evaluating the impact of this condition on both the healthcare system and patients. The findings may serve as a starting point for developing tailored preventive measures, optimizing therapeutic intervention strategies, and supporting vaccination and medical education initiatives among the general population and healthcare professionals.
Material and methods
The study was designed as an observational, descriptive, cross-sectional study during the years 1981-2013, aiming to assess the clinical-epidemiological characteristics and morbidity associated with recurrent laryngeal papillomatosis in the pediatric population of the Republic of Moldova. Ethical approval for the research was granted by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy, under decision no. 9, dated September 20, 2019.
The study analyzed data from 198 patients diagnosed with recurrent laryngeal papillomatosis who were admitted to the Emilian Coțaga Pediatric Otorhinolaryngology Clinic during the period 1981-2013.
The study included children up to 18 years old with a confirmed diagnosis of recurrent laryngeal papillomatosis. The diagnosis was established based on clinical and histopathological criteria. Patients with incomplete data or unconfirmed diagnoses were excluded.
The evaluation included demographic data (age, sex, and residence), medical and social factors, clinical details (age at disease onset, lesion sites), and epidemiological metrics (incidence and prevalence). The progression of the disease was followed for each patient over a period varying between 1 and 15 years.
The study was organized into clearly defined stages: setting objectives, selecting the sample, collecting data through medical records and questionnaires, processing and statistically analyzing the information, synthesizing the results, and formulating conclusions with practical applicability. Comparative analyses of demographic, geographic, and temporal data were performed to reveal key trends and disparities.
Data processing was performed using Microsoft Excel and Python (Jupyter Notebook) software. Both descriptive and inferential statistical methods were applied. Quantitative indicators were expressed using the arithmetic mean (M), median (Me), and mode (Mo).
The Shapiro-Wilk test was applied to assess the normality of the data distribution. Relationships between variables were examined using linear regression, a model that allows the evaluation of dependence between a scalar response and multiple independent variables.
Values of p < 0.05 were considered statistically significant, with results reported alongside 95% confidence intervals.
The results were organized into tables, graphs (histograms), and charts (including structural, column, and bar charts). Typological and variation analyses were performed based on the grouping of key indicators.
Results
Figure 1 presents a descriptive analysis of the variables included in the study, providing a detailed overview of the statistical distribution of each evaluated indicator. This enables not only the individual interpretation of the analyzed parameters but also a comprehensive understanding of the relationships among them, highlighting the relevance and consistency of the collected data.
The dataset is complete, comprising 198 observations for each analyzed variable, with no missing values. The average annual number of newly diagnosed cases is 6, with a peak of 15 cases reported in two separate years. The average number of annual medical visits is approximately 30, the majority of which involve male patients. The internal distribution of variables shows a relatively balanced statistical measure distribution between sexes. Disease progression extending into adulthood was not reported in any cases. The estimated prevalence of recurrent laryngeal papillomatosis among children is approximately 4.2 per 100,000.
|
Fig. 1 Frequency of new cases between 1991-2013 Note: Each block represents a calendar year, plotted against the number of newly diagnosed cases. The absence of pronounced fluctuations supports the hypothesis of a stable incidence over time, with no apparent cyclical or seasonal patterns. |
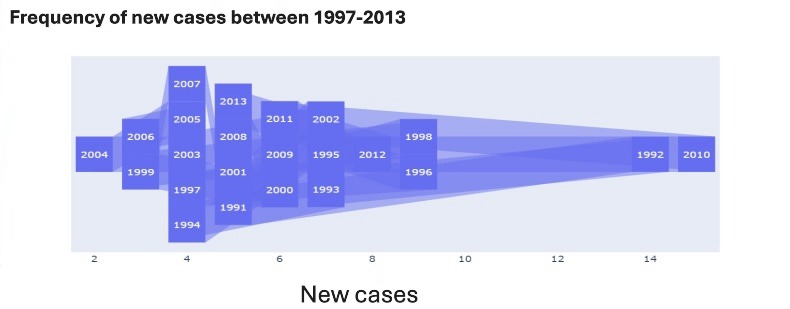
A retrospective analysis of cases of laryngeal papillomatosis in children in the Republic of Moldova during the period 1991-2013 reveals a fluctuating evolution, characterized by alternating episodes of increased incidence and periods of significant case decline (Fig. 1).
The highest incidence was recorded in 1991, with a total of approximately 15 cases, representing an early peak in the studied timeframe. After this point, the number of cases progressively decreased until 1994-1995, when a slight increase was observed. Another notable rise occurred around 1999, followed by a relatively steady decline in the early 2000s.
A minimum point on the curve was recorded between 2004 and 2006, when the number of cases remained below 5 per year. This relatively calm period was followed by a sudden resurgence starting in 2007, culminating in a second major epidemiological peak in 2010, when incidence again reached approximately 15 cases. Afterward, a slight decrease was noted, although the number of cases remained above the previous decade’s average until 2013.
This uneven evolution suggests the possible influence of cyclical or contextual contributing factors, such as a lack of national human papillomavirus vaccination program, the absence of active human papillomavirus screening in pregnant women, limited access to pediatric Otolaryngology care, and potentially underreporting of cases during certain periods.
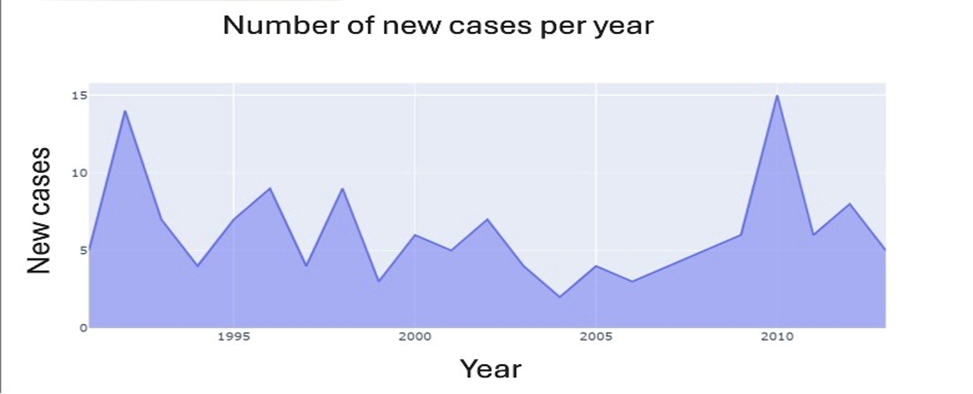 |
Fig. 2 The distribution of cases per year. Note: The graph shows the temporal distribution of new cases over the analyzed period, highlighting interannual variations without a consistent upward or downward trend. Isolated fluctuations may be attributed to reporting factors, access to care, or local epidemiological particularities. |
The annual distribution of medical consultations for recurrent laryngeal papillomatosis throughout the study period is illustrated in the figure (Fig. 2). Trend analysis highlights that the year 2004 recorded the lowest number of cases, while 2010 saw a peak with a total of 15 reported cases, indicating considerable variation in incidence over time.
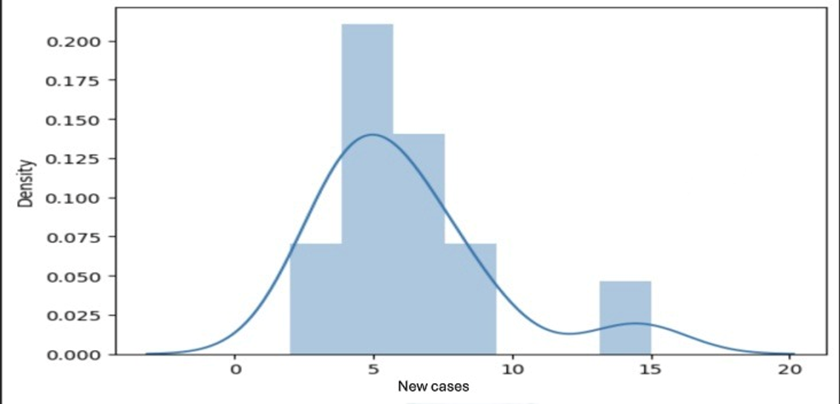 |
Fig. 3 Annual trend of reported recurrent laryngeal papillomatosis cases (1991–2013). Note: The distribution of newly reported cases follows a unimodal, right-skewed pattern, with most years clustering around 5 to 7 cases and a small number of outlier years exceeding 15 cases. This suggests a stable baseline incidence, occasionally interrupted by sporadic peaks. |
The annual progression of recurrent laryngeal papillomatosis cases during the study period is illustrated in the figure (Fig. 3). On average, the number of consultations per year remained below 9 cases. However, specific years – such as 1992 and 2010 – demonstrated a notable increase in frequency, reaching approximately 50% above the average. These isolated spikes, which lack a consistent temporal pattern, may indicate the influence of contextual or environmental factors on disease dynamics. Further investigation into these peaks could yield important insights into epidemiological behavior and inform the development of targeted preventive strategies.
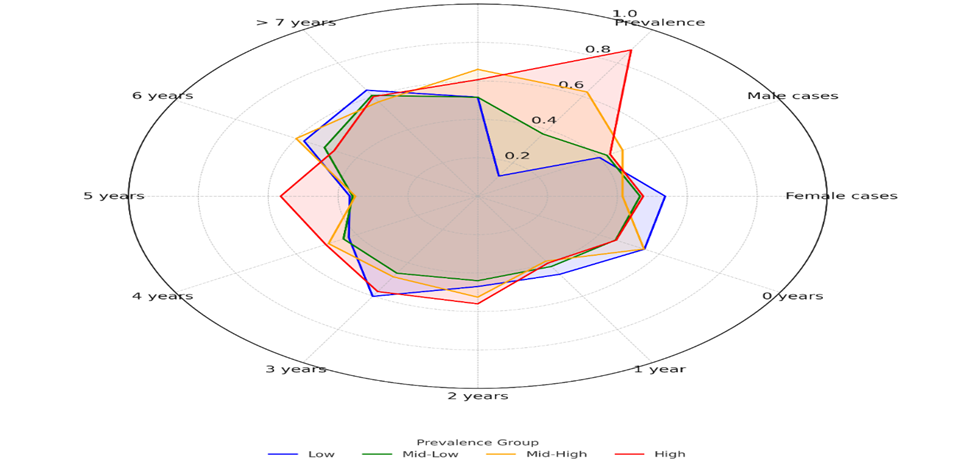 |
Fig. 4 Correlation between sex, age groups, and the number of new recurrent laryngeal papillomatosis cases Note: Radar chart illustrating the normalized median values of selected clinical and demographic variables stratified by four prevalence groups of recurrent laryngeal papillomatosis. Prevalence groups were defined by quartiles of the total prevalence distribution: Low (blue), Mid-Low (green), Mid-High (orange), and High (red). Variables include the number of new cases, overall prevalence, sex distribution (male and female), and age-specific representation from 0 to >7 years. The chart highlights distinct patterns across prevalence strata, with higher values in specific age groups and among males in high-prevalence clusters. |
In our study, a strong correlation (r = 0.86) was found between “Boys’ Cases” and “New Cases,” indicating that most new referrals originated from male patients (Fig. 4). Additional correlations between the “1 year” and “4 years” age groups suggest a higher frequency of disease onset at these ages, particularly among boys. Meanwhile, a moderate correlation between “Girls’ Cases” and “New Cases” (r = 0.76) reflects a relatively balanced incidence across sexes, with slight age-dependent variations.
Additional correlation analysis reveals a notable association (r = 0.63) between overall prevalence and the “4 years” age group, confirming a higher frequency of cases at this age among boys. Overall, the data suggest a concentration of cases around the ages of 1 and 4 for males, while in females, referrals tend to be more frequent between 7 and 15 years. These observations may be important for understanding the age and sex distribution of laryngeal papillomatosis onset and can help guide early interventions.
In our study, a strong correlation was observed between the number of new cases and the reported incidence per 100,000 population. However, this association may be considered misleading, as the incidence rate is directly calculated from the number of new cases. As a result, these two variables are not statistically independent, and the inclusion of incidence in a separate inferential analysis would not provide additional value.
The Shapiro-Wilk normality test applied to the distribution of new cases in our dataset demonstrated a balanced distribution between sexes, with no significant differences in the frequency of referrals. Nonetheless, a sex-based difference was noted regarding the age at presentation, suggesting a potential influence of gender on the timing of disease onset. This aspect merits further investigation in future research.
In our study, the evaluation of errors obtained through the linear regression method supports the validity of the previous interpretations. The estimated difference between the distribution of referrals for boys and girls compared to the total number of new cases is approximately ±2 cases. Furthermore, the predictive model based on these variables can estimate the number of new cases with a maximum deviation of ±7 cases from the actual data. However, developing a robust and reliable predictive model for forecasting future cases requires a larger sample size and more extensive data collection.
The analysis of statistical coefficients derived from linear regression in our study reveals that variables related to sex distribution (boys and girls) hold the most significant relevance for analyzing and predicting new cases in the upcoming period. While other variables contribute to a deeper understanding of the studied sample, they do not provide sufficient information for extrapolation to a broader theoretical population. Nonetheless, these variables remain valuable for the specific description and interpretation of the patient group included in our study.
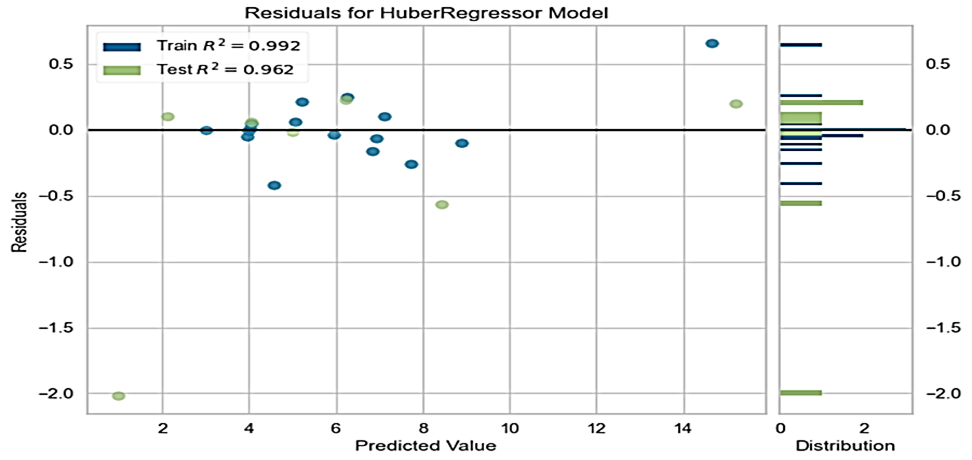 |
Fig. 5 Exploratory graphical assessment of residual distribution and variance stability in the predictive model Note: The figure displays residual values plotted against predicted values for both training (blue) and test (green) datasets. The residuals are mostly centered around zero, with minimal dispersion, indicating good model fit and stability. The distribution histogram (right) confirms the symmetrical spread of residuals, with isolated deviations below −2 in the test set. |
The error analysis resulting from the linear regression test applied to the predictive model demonstrates an approximately 90% homoscedastic distribution of errors, indicating that the variance of the residuals remains constant across the range of predicted values (Fig. 5). This consistency in error variance is essential for the validity of linear regression assumptions and ensures that coefficient estimates are efficient and unbiased. Consequently, the model proves to be robust, minimizing the risk of systematic errors in its predictions. However, for improved accuracy and generalizability, further analyses are recommended to identify any potential outliers or heteroscedasticity within specific data subsets.
Discussion
Recurrent laryngeal papillomatosis is a condition with significant clinical and social implications, especially among children, where disease recurrence and airway involvement can lead to severe complications. The present study, focused on the epidemiological and clinical analysis of pediatric patients in the Republic of Moldova, provides valuable insight into how this disease manifests and progresses within a specific regional context. The results align with recent global observations while also offering new data useful for planning clinical and public health interventions.
One of the most important findings of our study is the confirmation of a higher prevalence of recurrent respiratory papillomatosis (RRP)among boys compared to girls, a trend also reported in the international literature [15, 16]. The biological explanations for this sex difference remain under investigation; however, recent data suggest that immune response and susceptibility to human papillomavirus types 6 and 11 infections may be differently modulated based on sex [17, 18]. These variations may influence both the frequency of infection and the severity of clinical manifestations. Additionally, socio-cultural factors and differential access to healthcare services may play an important role in case detection and reporting, as highlighted by studies emphasizing inequalities within healthcare systems [19].
The average age at disease onset, around 1 and 4 years, aligns with the range reported in numerous multicenter studies [20, 21], suggesting a universal pattern of recurrent laryngeal papillomatosis progression in the pediatric population. These ages coincide with critical periods in immune system development and may reflect a window of increased vulnerability to initial human papillomavirus infection.
The average annual incidence identified in our study – approximately 6 new cases per year – is comparable to values published for regions with similar epidemiological profiles [22, 23]. Annual variability, with significant peaks in certain years (e.g., 1992 and 2010), may be attributed to various factors such as changes in public health policies, variability in case reporting, or actual fluctuations in viral transmission.
An estimated prevalence of 4.2 per 100,000 children is an important indicator highlighting the need for sustained preventive interventions. Although human papillomavirus vaccination remains insufficiently implemented in many regions, it has demonstrated increased efficacy in reducing recurrent laryngeal papillomatosis incidence [24, 25]. Implementing and expanding vaccination programs represent a strategic priority, especially given that recurrent laryngeal papillomatosis is directly associated with infection by human papillomavirus types 6 and 11, which are included in broad-spectrum human papillomavirus vaccines.
The application of linear regression in our study allowed the identification of statistically significant variables for predicting new case occurrences, particularly those related to sex distribution. This confirms the critical role of demographic factors in disease progression. However, the limited sample size and the absence of detailed data on other factors – such as vaccination status or the presence of comorbidities – limit the capacity to develop complex and robust predictive models [26].
The importance of controlling homoscedasticity and validating models through error analysis is well emphasized in recent methodological studies, which recommend close attention to error variance consistency to ensure accurate estimates and valid interpretations [27]. Our models largely meet these criteria but also highlight the need for further analyses, potentially using machine learning methods or nonlinear models that can better capture data complexity.
Early diagnosis of recurrent laryngeal papillomatosis is crucial for preventing severe complications, which may include airway obstruction, acute respiratory failure, and the need for invasive interventions such as tracheotomy [28]. In this context, educating primary healthcare providers, especially pediatricians and family doctors, about the symptoms and risk factors of recurrent laryngeal papillomatosis is essential to reduce diagnostic delays.
Current clinical management of recurrent laryngeal papillomatosis relies on repetitive surgical interventions; however, the high rate of recurrences necessitates the use of adjuvant therapies. New antiviral and immunomodulatory treatments have shown promising results in reducing recurrence frequency and disease severity [28]. Nonetheless, access to these treatments may be limited in some regions, including the Republic of Moldova, underscoring the need for effective interdisciplinary collaboration and appropriate resource allocation.
Although our study provides important data, the retrospective design entails inherent limitations, such as potential data incompleteness and the inability to control certain variables. Additionally, the lack of detailed information on vaccination history and other environmental factors poses a barrier to comprehensive assessment of causes and risks associated with recurrent laryngeal papillomatosis.
To better understand the involved immunological mechanisms and the predictive potential of biomarkers, prospective and multicenter studies are indispensable [29]. Such studies could integrate molecular, immunological, and epidemiological assessments, providing a solid basis for developing personalized treatment and prevention strategies.
Moreover, expanding human papillomavirus vaccination programs and monitoring their impact on RRP incidence should be a priority in public health policy in the Republic of Moldova and other countries with similar epidemiological profiles [30].
Conclusions
Recurrent laryngeal papillomatosis in children remains a rare but impactful condition, with early onset and clear demographic predispositions that underline the importance of timely diagnosis and multidisciplinary care. Despite current efforts, significant gaps persist in understanding its pathogenesis and recurrence patterns, warranting further prospective and integrative research. Expanding Human Papillomavirus vaccination coverage stands out as a necessary public health intervention, with the potential to reduce both clinical burden and long-term socioeconomic impact.
Competing interests
None declared.
Authors’ contributions
Both authors conceived and designed the study, collected and analyzed the data, and drafted the manuscript. Both authors critically reviewed and approved the final version of the manuscript.
Informed consent for publication
Obtained.
Acknowledgements and funding
No external funding.
Ethics approval
Ethical approval was obtained from the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy, under decision no. 9, dated September 20, 2019.
Provenance and peer review
Not commissioned, externally peer review.
Authors’ ORCID IDs
Daniela Cernev – https://orcid.org/0000-0001-8388-0901
Vasile Cabac – https://orcid.org/0000-0003-4899-7375
References
Abramson AL,Steinberg BM, Winkler B. Laryngeal papillomatosis:clinical, histopathologic and molecular studies. Laryngoscope. 1987;97(6):678-85. doi: 10.1288/00005537-198706000-00005.
Cernev D, Cabac V. Noțiuni generale de epidemiologie, etiopatogenie și tratament în papilomatoza laringiană recidivantă [General notions of epidemiology, etiopathogenesis and treatment in recurrent laryngeal papillomatosis]. Bull Acad Sci Mold. Med Sci. 2021;(3):93-97. Romanian.
Cabac V. Papilomatoza recidivantă a laringelui la copil: aspecte epidemiologice [Epidemiological aspects of recurrent laryngeal papillomatosis in children]. Bull Acad Sci Mold. Med Sci. 2013;(4):230-234. Romanian.
Armstrong LR, Preston EJ, Reichert M, Phillips DL, Nisenbaum R, Todd NW, et al. Incidence and prevalence of recurrent respiratory papillomatosis among children in Atlanta and Seattle. Clin Infect Dis. 2000 Jul;31(1):107-9. doi: 10.1086/313914.
Carifi M, Napolitano D, Morandi M, Dall'Olio D. Recurrent respiratory papillomatosis: current and future perspectives. Ther Clin Risk Manag. 2015 May 5:11:731-8. doi: 10.2147/TCRM.S81825.
Cernev D, Cabac V. Recurrent papillomatosis of the larynx. Etiological aspects, risk factors and the prognosis of clinical evolution. A a review of literature. Merit Res J Med Med Sci. 2020;8(10):584-588.
Cuello G, Sánchez GI, Jaramillo R, Quintero K, Baena A, O’Byrne A, et al. Clinical characteristics and HPV type in recurrent respiratory papillomatosis in Colombia. Salud Publica Mex. 2013;55(4):416-420. doi: 10.21149/spm.v55i4.7226.
Cabac V, Scutelnic L. Papilomatoza laringelui la copil: aspecte clinico-epidemiologice [Epidemiological aspects of recurrent laryngeal papillomatosis in children]. Public Health Econ Manag Med (Chisinau). 2016;(2):157-160. Romanian.
Cernev D, Cabac V, Spinei L. Incidenţa și prevalenţa papilomatozei laringiene la copii în Republica Moldova [Incidence and prevalence of laryngeal papillomatosis in children in the Republic of Moldova]. ORL.ro. 2024;(64):14. Romanian.
Cabac V, Parfeni V, Pojoga L, Sandul A. Unele aspecte ale papilomatozei laringiene la copil [Some aspects of the laringian papilomatosis in children]. Scientific Annals of Nicolae Testemitanu SUMPh. Chișinau: Medicina; 2008. Vol. 4. p. 218-223. Romanian.
Draganov P, Todorov S, Todorov I. Identification of HPV DNA in patients with juvenile-onset recurrent respiratory papillomatosis using SYBR® Green real-time PCR. Int J Pediatric Otorhinolaryngol. 2006 Mar;70(3):469-73. doi: 10.1016/j.ijporl.2005.07.018.
Venkatesan NN, Pine HS, Underbrink MP. Recurrent respiratory papillomatosis. Otolaryngol Clin North Am. 2012 Jun;45(3):671-94. doi: 10.1016/j.otc.2012.03.006.
Katsenos S, Becker HD. Recurrent respiratory pap-illomatosis: a rare chronic disease, difficult to treat, with potential to lung cancer transformation: a propos of two cases and a brief literature review. Case Rep Oncol. 2011;4(1):162-171. doi: 10.1159/000327094.
Reeves WC, Ruparelia SS, Swanson KI, Derkay CS, Marcus A, Unger ER. National registry for juvenile onset recurrent respiratory papillomatosis. Arch Otolaryngol Head Neck Surg. 2003;129(9):976-82. doi: 10.1001/archotol.129.9.976.
Hoesli R, Wingo ML, Richardson BE, Bastian RW. Identification of 11 different HPV subtypes in adult patients with recurrent respiratory papillomatosis. Otolaryngol Head Neck Surg. 2020;163(4):785-90.doi: 10.1177/0194599820931817.
Fortes HR, von Ranke FM, Escuissato DL, Araujo Neto CA, Zanetti G, Hochhegger B, et al. Recurrent respiratory papillomatosis: a state-of-the-art review. Respir Med. 2017;126(116):116-21. doi: 10.1016/j.rmed.2017.03.030.
San Giorgi MR, van den Heuvel ER, Tjon Pian Gi RE, Brunings JW, Chirila M, Friedrich G, et al. Age of onset of recurrent respiratory papillomatosis: a distribution analysis. Clin Otolaryngol. 2016;41(5):448-53. doi: 10.1111/coa.12565.
Stamataki S, Nikolopoulos TP, Korres S, Felekis D, Tzangaroulakis A, Ferekidis E. Juvenile recurrent respiratory papillomatosis: still a mystery disease with difficult management. Head Neck. 2007;29(2):155-62. doi: 10.1002/hed.20491.
Seedat RY. Juvenile-onset recurrent respiratory papillomatosis diagnosis and management: a developing country review. Pediatric Health Med Ther. 2020;11:39-46. doi: 10.2147/PHMT.S200186.
Lepine C, Leboulanger N, Badoual C. Juvenile onset recurrent respiratory papillomatosis: what do we know in 2024? Tumour Virus Res. 2024:17. doi: 10.1016/j.tvr.2024.200281.
Seedat RY, Schall R. Age of diagnosis, incidence and prevalence of recurrent respiratory papillomatosis: a South African perspective. Clin Otolaryngol. 2018 Apr;43(2):533-537. doi: 10.1111/coa.13016.
Novakovic D, Cheng AT, Baguley K, Walker P, Harrison H, Soma M, Malloy M, Brotherton JM. Juvenile recurrent respiratory papillomatosis: 10-year audit and Australian prevalence estimates. Laryngoscope. 2016 Dec;126(12):2827-2832. doi: 10.1002/lary.26005.
Ovcinnikova O, Engelbrecht K, Verma M, Pandey R, Morais E. A systematic literature review of the epidemiology, clinical, economic and humanistic burden in recurrent respiratory papillomatosis. Respir Res. 2024 Dec 18;25(1):430. doi: 10.1186/s12931-024-03057-w.
Jacobsen IM, Carlander AF, Aakilde M, von Buchwald C. Trends in the incidence and prevalence of juvenile-onset recurrent respiratory papillomatosis following implementation of national HPV vaccination initiatives: a systematic review. Acta Otolaryngol. 2025 Jan;145(1):66-71.doi: 10.1080/00016489.2024.2431548.
Ivancic R, Iqbal H, deSilva B, Pan Q, Matrka L. Current and future management of recurrent respiratory papillomatosis. Laryngoscope Investig Otolaryngol. 2018;3(1):22-34. doi: 10.1002/lio2.132.
Welschmeyer A, Berke GS. An updated review of the epidemiological factors associated with recurrent respiratory papillomatosis. Laryngoscope Investig Otolaryngol. 2021;6(2):226-33. doi: 10.1002/lio2.521.
Lindeberg H, Elbrond O. Laryngeal papillomas: the epidemiology in a Danish subpopulation 1965-1984. Clin Otolaryngol Allied Sci. 1990;15(2):125-31. doi: 10.1111/j.1365-2273.1990.tb00444.x.
Omland T, Akre H, Vardal M, Brondbo K. Epidemiological aspects of recurrent respiratory papillomatosis: a population-based study. Laryngoscope. 2012;122(7):1595-9. doi: 10.1002/lary.23327.
Oh JK, Choi HY, Han M, Jung YS, Lee SJ, Ki M. Estimated incidence of juvenile-onset recurrent respiratory papillomatosis in Korea. Epidemiol Health. 2021:43:e2021019. doi: 10.4178/epih.e2021019.
Yiu Y, Fayson S, Smith H, Matrka L. Implementation of routine HPV vaccination in the management of recurrent respiratory papillomatosis. Ann Otol Rhinol Laryngol. 2019;128(4):309-15. doi: 10.1177/0003489418821695.