

Introduction
Refractive Lens Exchange (RLE) is becoming an increasingly popular procedure, especially for individuals who are not suitable candidates for keratorefractive surgeries. It is particularly considered for patients with high degrees of myopia or hyperopia. However, the widespread availability of phacoemulsification devices and the growing number of surgeons trained in this technique have led to a reduction in the minimum age at which RLE is performed [1].
Case presentation
A 45-year-old female patient, B., presented to the Eye Microsurgery Ophthalmologic center in Moldova, with complaints of decreased visual acuity in the left eye (OS) for the past 9–10 days. Ophthalmologic history revealed that the patient had undergone clear lens phacoemulsification with monofocal IOL (Alcon Acrysof IQ) implantation in both eyes one year earlier. The ophthalmological examination findings are presented below in Table 1.
Table 1. Physical examination and instrumental data | ||
| OD | OS |
UDVA | 0.35 | 0.01 |
BDVA | 0.75 | 0.01 |
Autorefraction | -2.00 D sph / -0.75 D cyl ax 5 | -1.50 D sph / -1.25 D cyl ax 43°
|
Tonometry | 17 mmHg | 18 mmHg |
Biometry | 29.97 mm | 28.3 mm |
Biomicroscopy | Normal conjunctiva, white pearly sclera, clear smooth cornea, medium-depth anterior chamber, round reactive pupils, normal iris stroma, centered IOLs. | Normal conjunctiva, white pearly sclera, clear smooth cornea, medium-depth anterior chamber, round reactive pupils, normal iris stroma, centered IOLs. |
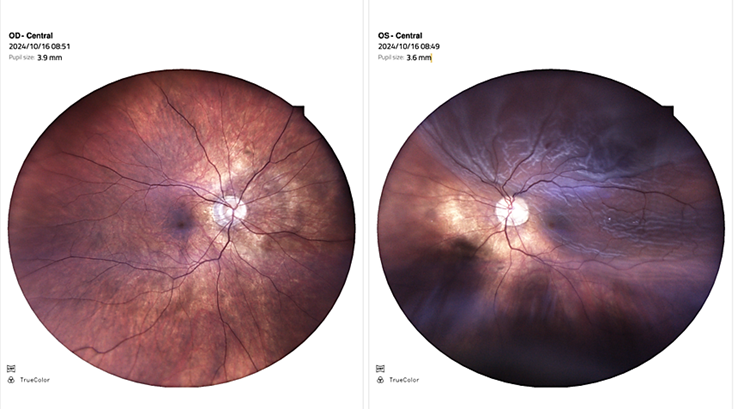
Fundus Examination | Flat, well-defined optic disc, mild peripapillary atrophy, C/D = 0.4, diminished macular reflex, moderately narrowed arteries and dilated veins, mobile vitreous opacities. | Superior sectorial retinal detachment, macula off (Figure 1) |
Note: OD - Right eye; OS - Left eye; UDVA - Uncorrected distance visual acuity; BDVA - Best corrected distance visual acuity; IOL - Intraocular lens; C/D - Cup/disc ratio. | ||
|
Fig. 1 Fundus photo at initial visit OD – Retina is attached, peripapillary atrophy, macular reflex is attenuated. |
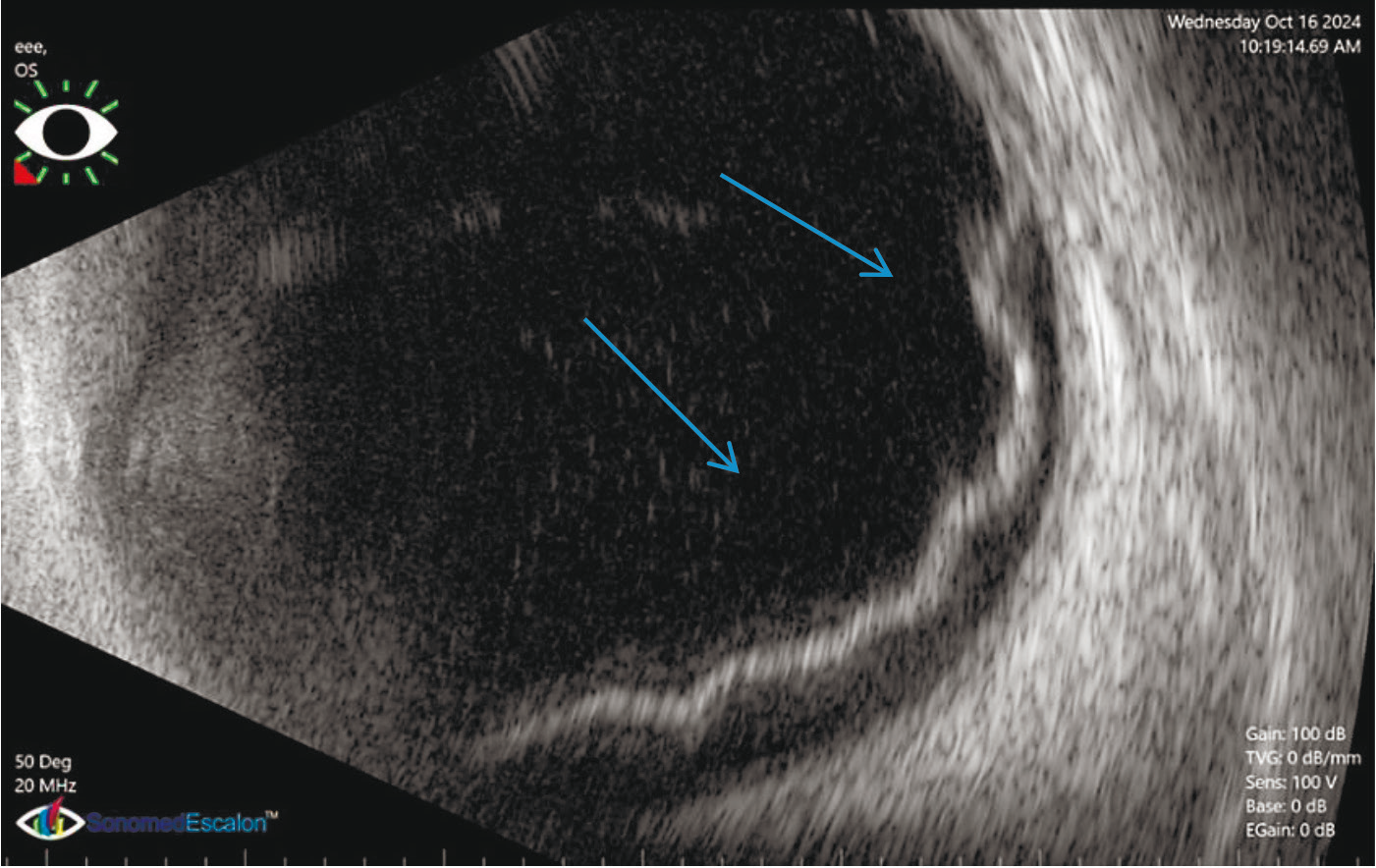
An ultrasound examination of the left eye was performed shown on Figures 2 & 3.
 |
|---|
Fig. 2 OS B-scan OS Retinal detachment (blue arrows). |
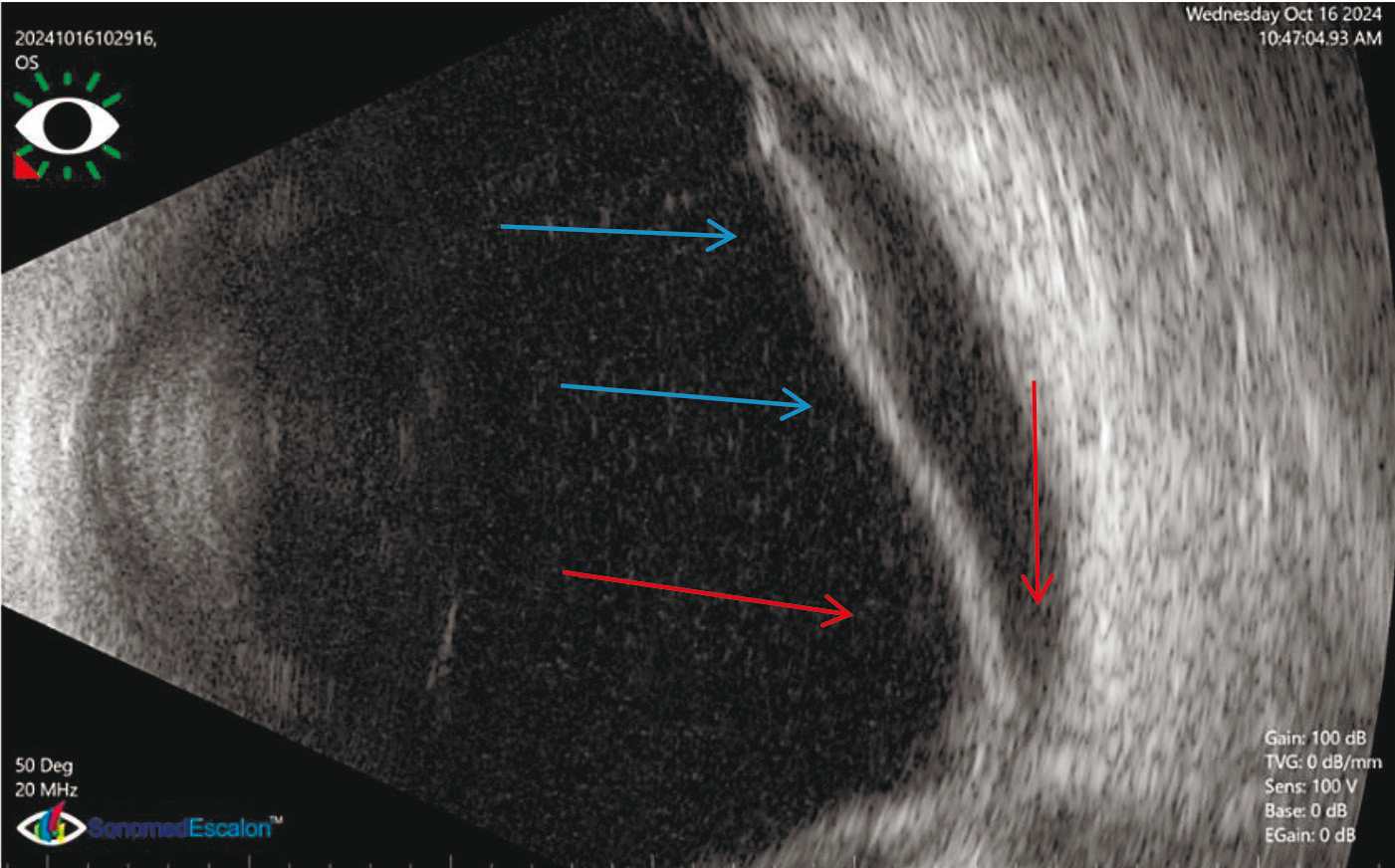 |
Fig. 3 OS B-scan OS Retinal detachment (blue arrows), optic disc (red arrows). |
The patient was diagnosed with OS: Rhegmatogenous retinal detachment, macula off; OU: Pseudophakia (postoperative high myopia), status post RLE and vitreous body degeneration.
Vitrectomy with endolaser photocoagulation and silicone oil tamponade was performed in the left eye (OS).
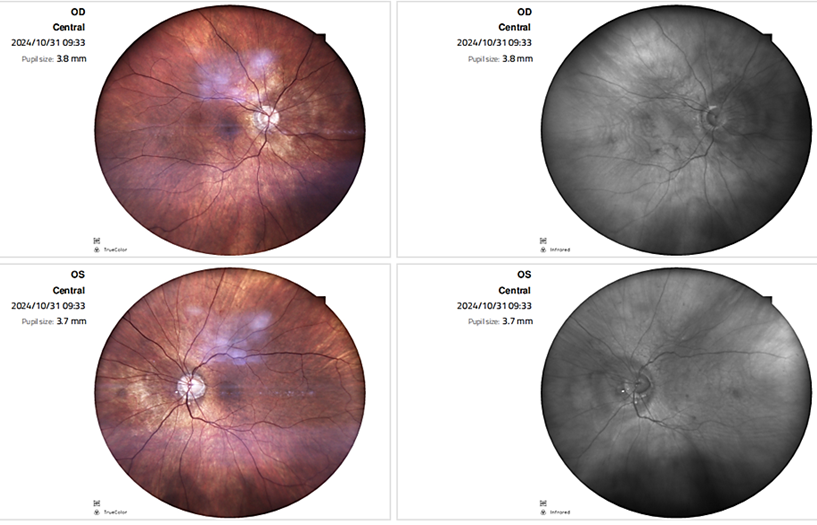
Postoperative follow-up (after 2 weeks) revealed OS BDVA of 0.3 and fundus examination (OS) with showed the retina reattached (Figure 4).
|
Fig. 4 Fundus photo OS Retina attached under silicone oil |
Discussion
One of the main considerations when evaluating refractive lens exchange (RLE) is the timing of posterior vitreous detachment (PVD). Patients with high myopia tend to develop PVD at a younger age compared to those without significant myopia.
Retinal detachment (RD) after RLE in highly myopic patients has been reported with an overall prevalence between 1.5% and 8.1%, depending on follow-up duration in various studies [1]. For comparison, the annual incidence of RD in the general population with high myopia is around 0.102%.
RD after RLE may be linked both to a predisposing factor (a higher prevalence of peripheral retinal lesions in highly myopic eyes) and a triggering factor (vitreous changes induced by the surgical procedure). Younger patients, especially those with an axial length greater than 26 mm (typically associated with myopia > -6.00 D), are at increased risk. The group with the highest risk includes patients under the age of 50 with an axial length exceeding 28 mm [1].
According to several sources, myopic eyes have a threefold higher risk of RD compared to the general cataract population [2].
Retinal complications – particularly in highly myopic eyes after refractive surgeries like RLE are primarily attributed to two main causes:
a higher incidence of predisposing peripheral retinal lesions in myopic eyes, and
the hypothesis that refractive surgery may induce certain iatrogenic factors increasing the incidence of such pathology [1, 3].
To prevent retinal detachment, careful preoperative fundus examination with scleral depression is necessary to assess the vitreous body. During surgery, minimal disturbance of the intraocular environment is essential. Some authors recommend bimanual microincision phacoemulsification (BMMI) or small-incision lens extraction in myopic eyes [1, 4].
During lens implantation, a transient drop in intraocular pressure (decompression effect) can lead to changes in the vitreous, particularly in eyes with existing vitreous degeneration. Protein alterations identified in pseudophakic eyes often coincide with structural changes in the vitreous body, which may contribute to the development of retinal complications postoperatively.
Preoperative determination of retinal detachment risk – especially in myopic eyes with axial length over 26.0 mm and spherical equivalent greater than -6.00 D – is of high importance [1, 5]. In young myopic patients, clear lens extraction may trigger vitreous changes and retinal traction not commonly seen in older patients undergoing age-related cataract surgery [1].
Conclusions
RLE is an intraocular surgical procedure that must be performed with precision and high accuracy. The indication for this intervention is the presence of a significant refractive error in the absence of cataract, and it requires a risk-benefit approach, taking into account the patient's age, refractive condition, and preoperative status. It is important to inform patients about the possible complications.
Competing interests
None declared.
Authors’ contributions
SP conducted the preoperative and postoperative assessment of the patient and collected the clinical data and performed the literature review. IT structured the article, drafted the conclusions. AP reviewed and revised the manuscript and recommended relevant literature to support the conclusions. All authors reviewed the manuscript critically and approved the final version.
Informed consent for publication
Obtained.
Acknowledgements and funding
We thank the Eye Microsurgery Ophthalmologic Center in Moldova, Chișinău, Republic of Moldova, for granting permission to conduct the clinical work. The study had no external funding.
Provenance and peer review
Not commissioned, externally peer review.
Authors’ ORCID IDs
Serghei Porada – https://orcid.org/0009-0000-7476-3527
Iulia Tanurcova – https://orcid.org/0009-0000-2242-1699
Ala Paduca – https://orcid.org/0000-0002-9879-8211
References
Alio JL, Pederzolli M, Grzybowski A. Refractive lens exchange: What are the red lines? Eur J Ophthalmol. 2024 Mar;34(2):317-322. doi: 10.1177/11206721231218909.
Rosen ES. Risk management in refractive lens exchange. J Cataract Refract Surg. 2008 Oct;34(10):1613-4. doi: 10.1016/j.jcrs.2008.08.001.
Ruiz-Moreno JM, Alio JL, Shabayek MH. Complications of refractive lens exchange. In: Alio JL, Azar DT, editors. Management of complications in refractive surgery. Berlin: Springer; 2008. p. 266-269.
O'Brien TP, Awwad ST. Phakic intraocular lenses and refractory lensectomy for myopia. Curr Opin Ophthalmol. 2002;13(4):264-270. doi: 10.1097/00055735-200208000-00015.
Alio JL. Lens surgery (cataract and refractive lens exchange) and retinal detachment risk in myopes: still an issue? Br J Ophthalmol. 2011;95(3):301-303. doi: 10.1136/bjo.2010.186429.