

Introduction
Obesity is a growing global health challenge, affecting millions of individuals worldwide [1, 2]. It results from a chronic imbalance between energy intake and expenditure, leading to excessive accumulation of adipose tissue [3]. Adipose tissue is now recognized as a metabolically active endocrine organ due to its ability to secrete a wide array of bioactive molecules with cytokine-like properties, collectively known as adipokines [4, 5]. Beyond their role in inflammation, these adipokines are involved in the regulation of appetite, body weight, insulin sensitivity, immune function, and the reproductive axis. Moreover, they play a pivotal role in the intricate control of bone function [6, 7]. Recent research has highlighted a bidirectional crosstalk between bone and energy homeostasis, pointing to osteocalcin, a bone-specific hormone, as a key player in this process. Produced by osteoblasts, osteocalcin is secreted into the peripheral circulation and promotes glucose uptake, participates in insulin signal transduction, and thus regulates energy metabolism in the whole body [8-10].
Several studies have examined the interplay between serum osteocalcin and body mass index (BMI), consistently reporting an inverse association [9, 11-14]. However, there is limited evidence regarding how circulating osteocalcin correlates with metabolic dysfunction and adiposity-related factors, particularly in young individuals with obesity. Given osteocalcin’s role in regulating glucose homeostasis, lipid metabolism, and insulin sensitivity, further investigation in this population may offer valuable insights into the early identification of biomarkers for cardiometabolic risk. Therefore, the aim of this study was to investigate the relationship between circulating osteocalcin levels and key metabolic parameters in young women living with obesity.
Material and methods
A cross-sectional observational study was conducted to explore the relationship between circulating osteocalcin levels and metabolic parameters in a sample of young women living with obesity. This study was carried out at the Department and Laboratory of Endocrinology, Nicolae Testemițanu State University of Medicine and Pharmacy, in the Republic of Moldova. Written informed consent was secured from all participants before enrolling in the study. Ethical approval was obtained from the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (minutes No.4, dated November 4, 2016).
A total of 85 young women, aged 18-45 years, with no history of illness or use of medication, were included in the study. The exclusion criteria were as follows: age under 18 or over 45 years, underweight women (BMI ≤ 18,5 kg/m²), overweight women (BMI 25-29.9 kg/m²), obesity secondary to other diseases, presence of comorbidities, menopause (natural, induced, or primary ovarian insufficiency), pregnancy or breastfeeding, individuals who refused to participate in the clinical study.
Anthropometric measurements, blood pressure and metabolic parameters were assessed for each participant using standardized procedures and calibrated equipment. BMI was calculated as weight in kilograms divided by the square of height in meters (kg/m²) [2]. Waist circumference (WC) was measured at the umbilicus using a measuring tape [2]. Hip circumference (HC) was measured around the most prominent area of the buttocks [15]. The waist-to-hip ratio (WHR) and waist-to-height ratio (WHtR) were calculated, based on standard measurement protocols.
Blood pressure was measured with participants seated comfortably after a 5-minute rest, using a calibrated sphygmomanometer.
For laboratory evaluations, venous blood samples were collected in the morning following a 10-hour overnight fast. Serum concentrations of osteocalcin, adiponectin, glucose, insulin, total cholesterol, low-density lipoprotein cholesterol (LDL-cholesterol), and high-density lipoprotein cholesterol (HDL-cholesterol) were measured using standard automated techniques. Insulin resistance was assessed using the Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) and the Quantitative Insulin Sensitivity Check Index (QUICKI) [16, 17].
All statistical analyses were performed using the GNU PSPP (Version 2.0.1) software package. Continuous variables were presented as mean (standard deviation (SD)). Comparisons between the obesity group (BMI ≥ 30 kg/m²) and the normal weight group (BMI 18.5-24.9 kg/m²) were analyzed using ANOVA. Pearson correlation analysis was used to evaluate the linear relationship between osteocalcin levels and anthropometric, hemodynamic, and metabolic parameters. Statistical significance was set at p < 0.05 for all analyses.
Results
According to the eligibility criteria, 85 young Caucasian women (mean age 31.92 (6.72) years) were included in the study. Based on their BMI, participants were categorized into two study groups: L0 – 47 women with normal weight (BMI 18.5–24.9 kg/m²), and L1 – 38 women with obesity (BMI ≥ 30 kg/m²).
Table 1 summarizes the anthropometric, hemodynamic, and metabolic characteristics of the study population by BMI category. No significant difference was observed in age between the two groups (p = 0.338), indicating appropriate age matching.
Table 1. Clinical characteristics of the study population by BMI category (mean (SD)). | ||||
Variables | Total n = 85 | BMI 18.5-24.9 kg/m2, n = 47 (L0) | BMI ≥ 30 kg/m2, n = 38 (L1) | p-value |
Age | 31.92 (6.72) | 31.2 (6.22) | 32.68 (7.24) | 0,338 |
Weight, kg | 80.04 (22.32) | 61.63 (6.49) | 99.43 (15.89) | ˂ 0.001 |
BMI, kg/m2 | 28.6 (7.5) | 22.01 (1.85) | 35.55 (4.30) | ˂ 0.001 |
WHR, cm | 0.86 (0.07) | 0.82 (0.06) | 0.92 (0.05) | ˂ 0.001 |
WHtR, cm | 0.56 (0.12) | 0.46 (0.04) | 0.67 (0.06) | ˂ 0.001 |
SBP, mmHg | 116.28 (10.27) | 112.5 (10.31) | 120.26 (8.85) | ˂ 0.001 |
DBP, mmHg | 72.5 (6.59) | 69.88 (6.75) | 75.26 (5.32) | ˂ 0.001 |
Osteocalcin, ng/mL | 16.46 (5.51) | 19.75 (4.09) | 12.99 (4.7) | ˂ 0.001 |
Adiponectin, μg/mL | 20.15 (15.5) | 28.98 (15.28) | 10.86 (9.48) | ˂ 0.001 |
Fasting glucose, mmol/L | 4.82 (0.63) | 4.66 (0.54) | 4.98 (0.69) | = 0.022 |
Insulin, µU/mL | 10.18 (6.56) | 6.47 (2.59) | 14.07 (7.29) | ˂ 0.001 |
HOMA-IR | 2.23 (1.63) | 1.33 (0.56) | 3.17 (1.86) | ˂ 0.001 |
QUICKI | 0.35 (0.03) | 0.37 (0.03) | 0.33 (0.02) | ˂ 0.001 |
Total cholesterol, mmol/L | 5.28 (0.72) | 5.01 (0.61) | 5.56 (0.75) | ˂ 0.001 |
LDL-cholesterol, mmol/L | 2.55 (0.81) | 1.95 (0.45) | 3.18 (0.61) | ˂ 0.001 |
HDL-cholesterol, mmol/L | 1.74 (0.37) | 1.89 (0.25) | 1.57 (0.41) | ˂ 0.001 |
Note: Data are presented as mean (standard deviation, SD). BMI – body mass index; WHR – waist-to-hip ratio; WHtR – waist-to-height ratio; SBP – systolic blood pressure; DBP – diastolic blood pressure; HOMA-IR – homeostasis model assessment of insulin resistance; QUICKI – quantitative insulin sensitivity check index; LDL – low-density lipoprotein; HDL – high-density lipoprotein. The study population was divided into two groups according to BMI: normal weight (L0, 18.5–24.9 kg/m²) and obesity (L1, ≥30 kg/m²). Groups were compared using ANOVA procedure. A p-value <0.05 was considered statistically significant. | ||||
As expected, women with obesity (L1, BMI ≥ 30 kg/m²) had significantly higher mean body weight and BMI compared to the normal-weight group (L0, BMI 18.5-24.9 kg/m2). Central adiposity markers, including waist-to-hip ratio (WHR) and waist-to-height ratio (WHtR), were also significantly elevated in the L1 group (p < 0.001), reflecting increased visceral fat accumulation.
Hemodynamic parameters differed significantly between groups. Both SBP and DBP were higher in the L1 group (p < 0.001), indicating a trend toward elevated cardiovascular risk in women with obesity.
Regarding biochemical parameters, serum levels of osteocalcin and adiponectin were significantly lower in the L1 group compared to L0 (p < 0.001 for both), suggesting hormonal dysregulation associated with increased adiposity.
Markers of glucose metabolism showed significant group differences. Women with obesity exhibited higher fasting glucose (p = 0.022), insulin (p < 0.001), and HOMA-IR values (p < 0.001), while QUICKI was significantly lower (p < 0.001), indicating decreased insulin sensitivity.
Lipid profile analysis revealed a more atherogenic pattern in the L1 group, with significantly higher total cholesterol and LDL cholesterol, and lower HDL cholesterol levels (p < 0.001 for all).
These findings highlight the presence of significant metabolic, hormonal, and cardiovascular alterations in young women with obesity, supporting the hypothesis that increased adiposity is associated with dysregulation of both classic cardiometabolic markers and bone-derived hormones such as osteocalcin.
Table 2. Pearson correlation between serum osteocalcin, adiponectin and anthropometric, metabolic, and cardiovascular parameters in the total study population (n = 85) | ||||
Variables | Osteocalcin | Adiponectin | ||
r | p-value | r | p-value | |
BMI, kg/m2 | -0.56 | ˂ 0.001 | -0.48 | ˂ 0.001 |
WHR, cm | -0.54 | ˂ 0.001 | -0.50 | ˂ 0.001 |
WHtR, cm | -0.57 | ˂ 0.001 | -0.48 | ˂ 0.001 |
SBP, mmHg | -0.22 | = 0.040 | -0.24 | = 0.007 |
DBP, mmHg | -0.29 | = 0.007 | -0.29 | = 0.001 |
Osteocalcin, ng/mL | - | - | 0.31 | = 0.005 |
Adiponectin, μg/mL | 0.31 | = 0.005 | - | - |
Fasting glucose, mmol/L | -0.13 | = 0.237 | 0.47 | 0.590 |
Insulin, µU/mL | -0.37 | ˂ 0.001 | -0.45 | ˂ 0.001 |
HOMA-IR | -0.35 | ˂ 0.001 | -0.41 | ˂ 0.001 |
QUICKI | 0.39 | ˂ 0.001 | 0.48 | ˂ 0.001 |
Total cholesterol, mmol/L | -0.40 | ˂ 0.001 | -0.30 | ˂ 0.001 |
LDL-cholesterol, mmol/L | -0.54 | ˂ 0.001 | -0.48 | ˂ 0.001 |
HDL-cholesterol, mmol/L | 0.21 | 0.054 | 0.31 | ˂ 0.001 |
Note: Data are presented as Pearson correlation coefficients (r) with corresponding p-values. BMI – body mass index; WHR – waist-to-hip ratio; WHtR – waist-to-height ratio; SBP – systolic blood pressure; DBP – diastolic blood pressure; HOMA-IR – homeostasis model assessment of insulin resistance; QUICKI – quantitative insulin sensitivity check index; LDL – low-density lipoprotein; HDL – high-density lipoprotein. Correlations were assessed using the Pearson correlation test. A p-value <0.05 was considered statistically significant. | ||||
Table 2 presents Pearson correlation coefficients between serum osteocalcin and adiponectin levels and anthropometric, hemodynamic, and metabolic parameters.
Both osteocalcin and adiponectin showed strong negative correlations with indicators of adiposity, including BMI, WHR, and WHtR (all p < 0.001), indicating that lower concentrations of these hormones are associated with increased fat accumulation.
In terms of hemodynamic measures, both markers were inversely associated with SBP and DBP. The correlation was stronger for DBP (osteocalcin: r = –0.29, p = 0.007; adiponectin: r = –0.29, p = 0.001).
Regarding insulin resistance, both osteocalcin and adiponectin were negatively correlated with insulin and HOMA-IR (p < 0.001), and positively correlated with QUICKI (p < 0.001), suggesting their involvement in glucose homeostasis and insulin sensitivity.
For the lipid profile, both markers were negatively correlated with total cholesterol and LDL cholesterol, and positively associated with HDL cholesterol. The association with HDL cholesterol was statistically significant for adiponectin (p < 0.001) and borderline for osteocalcin (p = 0.054).
Additionally, a positive correlation was observed between osteocalcin and adiponectin themselves (p = 0.005), suggesting potential synergistic or complementary roles in metabolic regulation.
Further subgroup analysis of osteocalcin levels by obesity grade revealed a stepwise decline in concentrations with increasing adiposity (Fig. 1). The highest mean value was observed in the normal-weight group (20.10 ± 4.47 ng/mL). The lowest level occurred in women with grade I obesity (12.14 ± 4.84 ng/mL), while slightly higher values were recorded in those with grade II (14.24 ± 5.19 ng/mL) and grade III obesity (13.32 ± 2.97 ng/mL). These results further emphasize the inverse association between osteocalcin levels and the degree of adiposity.
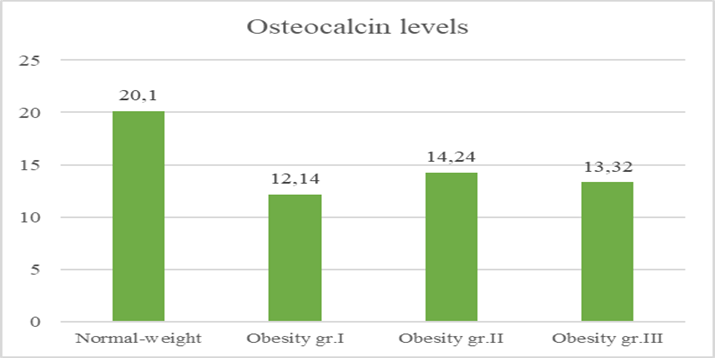 |
Fig. 1 Mean osteocalcin levels by weight category Note: Mean osteocalcin concentrations (ng/mL) are presented for normal-weight women and for those with obesity grades I–III. Data are shown as mean values. Group comparisons were performed using one-way ANOVA procedure. A p-value <0.05 was considered statistically significant. |
Discussion
This study examined the association between circulating osteocalcin levels and key metabolic markers in young women with obesity. Findings revealed that osteocalcin concentrations were significantly lower in women with obesity compared to those with normal weight. Furthermore, osteocalcin showed strong inverse correlations with measures of adiposity (BMI, WHR, WHtR), insulin resistance (insulin, HOMA-IR), and lipid disturbances (total and LDL cholesterol), while being positively correlated with insulin sensitivity as measured by QUICKI. A moderate positive correlation between osteocalcin and adiponectin was also observed, indicating possible complementary or synergistic functions in metabolic regulation.
These findings align with previous studies reporting an inverse association between osteocalcin and BMI, and expand current knowledge by revealing robust associations with metabolic and cardiovascular risk markers. In a meta-analysis of 28 studies comprising 18,630 participants aged 36 to 75.3 years, Kord-Varkaneh et al. (2017) confirmed a significant inverse relationship between serum osteocalcin and BMI in adult populations [11]. Similarly, Riquelme-Gallego et al. (2020) conducted a recent population-based study that investigated the association between total osteocalcin levels and obesity, hypertension, and type 2 diabetes. Their findings demonstrated that osteocalcin was significantly and negatively associated with BMI, waist circumference, and HbA1c, and positively associated with HDL cholesterol and systolic blood pressure [18].
Notably, most prior research on osteocalcin has focused on older adults, postmenopausal women, or individuals with established comorbidities such as type 2 diabetes, cardiovascular disease, or osteoporosis [18-23]. In contrast, the present study addresses an important gap by evaluating these associations in a metabolically active population of young women without overt chronic illness, thereby providing early insights into the role of bone-derived hormones in cardiometabolic health.
A key observation was the progressive decline in osteocalcin concentrations across obesity grades, reinforcing the concept of a reciprocal interaction between bone and energy metabolism and suggesting that osteocalcin may serve as a valuable early biomarker of metabolic dysregulation.
The biological plausibility of these findings is supported by experimental evidence showing that osteocalcin enhances insulin secretion and sensitivity, promotes glucose uptake, and regulates lipid metabolism [8, 10]. The observed positive correlation with adiponectin, a key insulin-sensitizing adipokine, further supports the role of osteocalcin in modulating endocrine and metabolic pathways.
This study has several strengths, including its focus on a relatively homogeneous and young cohort without comorbid conditions, and the comprehensive assessment of metabolic and hormonal parameters. However, some limitations should be noted. The cross-sectional design limits the ability to draw causal inferences, and the sample size, while sufficient for correlation analysis, may limit broader generalizability.
Future research should explore longitudinal associations to better understand osteocalcin’s dynamic role in metabolic regulation. Studies in larger, more diverse cohorts and interventional trials may help clarify the potential of osteocalcin as a predictive marker or therapeutic target in obesity-related metabolic dysfunction.
Conclusions
This study demonstrates that circulating osteocalcin levels are significantly reduced in young women with obesity and are strongly associated with key metabolic parameters, including indicators of adiposity, insulin resistance, and lipid abnormalities. The progressive decline in osteocalcin concentrations across obesity grades highlights its potential involvement in the early pathophysiology of metabolic dysfunction.
The observed inverse correlations with BMI, insulin, HOMA-IR, and LDL cholesterol, along with positive associations with insulin sensitivity (QUICKI) and adiponectin, suggest that osteocalcin may serve as a sensitive early biomarker of cardiometabolic risk in this population. These findings underscore the importance of a comprehensive and multifactorial approach to the assessment of individuals living with obesity to support earlier identification of at-risk individuals and more effective prevention of obesity-related complications.
Competing interests
None declared.
Authors’ contributions
LV conceived the study and participated in study design and helped drafting the manuscript. CP participated in the study design, performed the statistical analysis, and drafted the manuscript. Both authors reviewed the work critically and approved the final version of the manuscript.
Patient consent
Obtained.
Ethics approval
The study was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (minutes No. 4, dated 04.11.2016).
Acknowledgements and funding
No external funding.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Authors’ ORCID IDs
Carolina Piterschi – https://orcid.org/0009-0002-5459-1013
Lorina Vudu – https://orcid.org/0000-0002-7481-3843
References
Abad-Jiménez Z, Vezza T. Obesity: a global health challenge demanding urgent action. Biomedicines 2025;13(2):502. https://doi.org/10.3390/biomedicines13020502.
World Health Organization. Obesity and overweight 2024 [Internet]. Geneva: WHO; c2025- [cited 2025 May 13]. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
Jin X, Qiu T, Li L, Yu R, Chen X, Li C, et al. Pathophysiology of obesity and its associated diseases. Acta Pharm Sin B. 2023;13(6):2403-24. https://doi.org/10.1016/j.apsb.2023.01.012.
Kershaw EE, Flier JS. Adipose tissue as an endocrine organ. J Clin Endocrinol Metab. 2004;89(6):2548-56. https://doi.org/10.1210/jc.2004-0395.
Romacho T, Elsen M, Röhrborn D, Eckel J. Adipose tissue and its role in organ crosstalk. Acta Physiol. 2014;210(4):733-53. https://doi.org/10.1111/apha.12246.
Clemente-Suárez VJ, Redondo-Flórez L, Beltrán-Velasco AI, Martín-Rodríguez A, Martínez-Guardado I, Navarro-Jiménez E, et al. The role of adipokines in health and disease. Biomedicines. 2023;11(5):1290. https://doi.org/10.3390/biomedicines11051290.
Hemat Jouy S, Mohan S, Scichilone G, Mostafa A, Mahmoud AM. Adipokines in the crosstalk between adipose tissues and other organs: implications in cardiometabolic diseases. Biomedicines. 2024;12(9):2129. https://doi.org/10.3390/biomedicines12092129.
Moser SC, van der Eerden BCJ. Osteocalcin – a versatile bone-derived hormone. Front Endocrinol (Lausanne). 2019;10:794. https://doi.org/10.3389/fendo.2018.00794.
Smith C, Lin X, Parker L, Yeap BB, Hayes A, Levinger I. The role of bone in energy metabolism: a focus on osteocalcin. Bone. 2024;188:117238. https://doi.org/10.1016/J.BONE.2024.117238.
Zhou R, Guo Q, Xiao Y, Guo Q, Huang Y, Li C, et al. Endocrine role of bone in the regulation of energy metabolism. Bone Res. 2021;9(1):25. https://doi.org/10.1038/s41413-021-00142-4.
Kord-Varkaneh H, Djafarian K, khorshidi M, Shab-Bidar S. Association between serum osteocalcin and body mass index: a systematic review and meta-analysis. Endocrine. 2017;58(1):24-32. https://doi.org/10.1007/s12020-017-1384-4.
Nowicki JK, Jakubowska-Pietkiewicz E. Osteocalcin: beyond bones. Endocrinol Metabol. 2024;39(3):399-406. https://doi.org/10.3803/EnM.2023.1895.
Kanazawa I. Osteocalcin as a hormone regulating glucose metabolism. World J Diabetes. 2015;6(18):1345-54. https://doi.org/10.4239/wjd.v6.i18.1345.
Guedes JAC, Esteves J V, Morais MR, Zorn TM, Furuya DT. Osteocalcin improves insulin resistance and inflammation in obese mice: Participation of white adipose tissue and bone. Bone. 2018;115:68-82. doi: 10.1016/j.bone.2017.11.020.
Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser. 1995;854:1-452.
Katz A, Nambi SS, Mather K, Baron AD, Follmann DA, Sullivan G, et al. Quantitative insulin sensitivity check index: a simple, accurate method for assessing insulin sensitivity in humans. J Clin Endocrinol Metab. 2000;85(7):2402-10. https://doi.org/10.1210/jcem.85.7.6661.
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412-9. https://doi.org/10.1007/BF00280883.
Riquelme-Gallego B, García-Molina L, Cano-Ibáñez N, Sánchez-Delgado G, Andújar-Vera F, García-Fontana C, et al. Circulating undercarboxylated osteocalcin as estimator of cardiovascular and type 2 diabetes risk in metabolic syndrome patients. Sci Rep. 2020;10(1):1840. https://doi.org/10.1038/s41598-020-58760-7.
Pergola G, Triggiani V, Bartolomeo N, Nardecchia A, Giagulli V, Bruno I, et al. Independent relationship of osteocalcin circulating levels with obesity, type 2 diabetes, hypertension, and HDL cholesterol. Endocr Metab Immune Disord Drug Targets. 2017;16(4):270-5. https://doi.org/10.2174/1871530317666170106150756.
Sanchez-Enriquez S, Ballesteros-Gonzalez IT, Villafán-Bernal JR, Pascoe-Gonzalez S, Rivera-Leon EA, Bastidas-Ramirez BE, et al. Serum levels of undercarboxylated osteocalcin are related to cardiovascular risk factors in patients with type 2 diabetes mellitus and healthy subjects. World J Diabetes. 2017;8(1):11. https://doi.org/10.4239/wjd.v8.i1.11.
Viswanath A, Vidyasagar S, Amrutha Sukumar C. Osteocalcin and metabolic syndrome. Clin Med Insights Endocrinol Diabetes. 2023;16. https://doi.org/10.1177/11795514231206729.
Moon JS, Jin MH, Koh HM. Association between serum osteocalcin levels and metabolic syndrome according to the menopausal status of Korean women. J Korean Med Sci. 2021;36(8):e56. https://doi.org/10.3346/jkms.2021.36.e56.
Pattanayak N, Mishra A, Mohanty S, Mishra PK, Bara P. Association of osteocalcin with metabolic syndrome and its correlation with insulin resistance. J Clin Diagn Res. 2021;15(2):15-19. https://doi.org/10.7860/JCDR/2021/47063.14587.