

Introduction
Ovarian cancer remains the most lethal gynecologic malignancy worldwide [1, 2]. In 2022, approximately 324,600 new cases were recorded globally, and the 5-year relative survival rate remains only 51.6% in the United States, despite the availability of multimodal therapies [3, 4]. Around 90% of ovarian cancer cases are of epithelial origin, while the remaining 10% include non-epithelial forms such as sex cord-stromal tumors, germ cell neoplasms, and other rare carcinoma types [5-7].
According to the 2020 World Health Organization classification, epithelial ovarian carcinoma is divided into five main histologic subtypes: serous, mucinous, endometrioid, clear cell, and NOS-type (not otherwise specified) adenocarcinoma [6, 7]. High-grade serous tubo-ovarian carcinoma represents the most frequent and extensively studied form of ovarian cancer, accounting for approximately 70% of all cases [8]. In contrast, low-grade serous carcinoma is considered a rare entity, representing 2–5% of all ovarian malignancies and approximately 5–10% of serous carcinoma cases [9, 10]. Each histologic subtype displays distinct biological characteristics, is associated with different cellular origins and specific immunohistochemical markers, and facilitates both diagnostic accuracy and prognostic assessment. Advances in the molecular understanding of these tumors have opened new directions for developing targeted therapies; nevertheless, further studies are required to adapt treatment strategies to the features of each subtype [11].
Mutations in the BRCA1 and BRCA2 genes, as well as Lynch syndrome, are involved in up to 25% of cases [13, 14]. The disease exhibits a hormone-dependent component, and an imbalance between estrogen receptors ERα and ERβ – particularly the overexpression of ERα – plays an important role in the carcinogenesis process [15]. Protective factors include oral contraceptive use, pregnancy, breastfeeding, and tubal ligation, whereas endometriosis, a vegetable-poor diet, and in vitro fertilization procedures may increase the risk of developing the disease [12, 15, 16].
In the effort to identify prognostic and therapeutic biomarkers in serous ovarian carcinoma, research has focused on the expression of estrogen (ER) and progesterone (PR) hormone receptors [17, 18]. Recent evidence suggests that tumor hormonal status is not merely an immunohistochemical artifact but rather reflects meaningful biological traits: elevated PR expression is frequently associated with improved survival, while the prognostic role of ER remains ambiguous and appears to be context-dependent [19]. However, most studies addressing hormone receptors have been conducted in breast cancer, where compelling results have led to the development of effective endocrine therapies, demonstrating the clinical value of these markers [20, 21]. In contrast, the literature on serous ovarian carcinoma continues to reveal contradictory results, driven by cohort heterogeneity and the lack of consensus on positivity thresholds – such as the use of the Allred scoring system. Within this framework, methodological standardization becomes essential for clinical validation of hormone receptors and for adapting them to the specific context of ovarian oncology [22, 23].
The study hypothesizes that the immunohistochemical expression of estrogen (ER) and progesterone (PR) receptors in serous ovarian carcinoma influences disease progression and holds prognostic relevance. It is presumed that increased receptor expression is associated with a more favorable prognosis. The objective of the study is to evaluate ER and PR receptor expression through immunohistochemistry in serous ovarian carcinoma and to correlate expression levels with clinicopathological parameters, aiming to identify potentially useful markers for personalized oncologic treatment.
Material and methods
The study material consisted of tissue samples morphopathologically diagnosed with high-grade and low-grade serous ovarian carcinoma, collected from patients aged between 18 and 85 years. These specimens were retrieved from the archives of the Oncology Institute and Gheorghe Paladi Municipal Clinical Hospital, Chișinău, Republic of Moldova, during the period 2022–2024 and included in the final analysis. All patients underwent surgical procedures, including laparotomy or exploratory laparoscopy with biopsy, adnexectomy, total hysterectomy with bilateral adnexectomy, and tumor cytoreduction.
For external control in immunohistochemistry using anti-ER and anti-PR antibodies, breast carcinoma samples with confirmed hormone receptor expression were employed. Negative controls were performed by omitting the primary antibody, ensuring the specificity of the reaction. Relevant clinical data were collected from the medical records of the patients included in the study.
Histological examination methodology included standard processing of tissue samples, hematoxylin-eosin (H&E) staining, and application of immunohistochemical techniques using specific anti-ER and anti-PR antibodies. Morphological evaluation of immunohistochemical reactions was performed via microscopic analysis, followed by rigorous statistical processing of the obtained data.
Primary processing. Selected tissue specimens were immediately fixed in a 10% buffered formalin solution with a pH between 7.2 and 7.4, to prevent autolysis and microbial proliferation. Fixation time did not exceed 24 hours.
Histological processing was performed using the HistoCore PEARL tissue processor (Leica), followed by paraffin embedding with the Arcadia system (Leica). Tissue sectioning was carried out with the Biocut microtome (Leica), yielding 3–4 µm sections mounted on positively charged slides (Detalab, Spain), suitable for both histologic and immunohistochemical evaluation.
Histological technique. Slides were stained using the classical H&E method with the ST Infinity H&E Staining System (Leica). Automated staining was conducted using the ST5010 XL autostainer (Leica), and slide mounting was completed using the CV5030 system (Leica). Sections with adequate tissue material were selected for immunohistochemical staining.
Immunohistochemical technique. Immunostaining was performed using the BOND-MAX automated system (Leica), applying ready-to-use antibodies: BOND Estrogen Receptor (clone 6F11) and BOND Progesterone Receptor (clone 16). Detection was performed with the BOND Polymer Refine Detection system (Leica). The standard IHC-F protocol was applied as described in Table 1.
Table 1. Characteristics of primary antibodies used for immunohistochemistry. | |||
Antibody/clone | Source/incubation time/dilution | Retrieval system/time | Detection/time |
Er/6F11 | BOND/15 min /ready-to-use | BOND Epitope Retrieval Solution 1 / 20 min | BOND Polymer Refine Detection, Leica / 8 min |
Pr/16 | BOND/15 min/ ready-to-use | BOND Epitope Retrieval Solution 2 / 20 min | BOND Polymer Refine Detection, Leica/ 8 min |
Note: ER – estrogen receptor; PR – progesterone receptor. All antibodies were ready-to-use and applied according to manufacturer protocols. Data presented are categorical (qualitative) descriptions of IHC protocol parameters. | |||
Deparaffinization of sections was achieved by exposure to DEWAX solution and Histanol 100 (H100-118/20). Epitope retrieval involved treating the slides with BOND ER Solution 1 (low pH) for ER and BOND ER Solution 2 (high pH) for PR antibodies, at 97–98°C for 20 minutes. Endogenous peroxidase neutralization was performed using BOND Peroxide Block for 5 minutes.
Primary antibody incubation lasted 15 minutes at room temperature for each antibody. BOND Post Primary and BOND Polymer reagents were applied for 8 minutes each. DAB (3,3′-diaminobenzidine) was used as the chromogen substrate, applied for 10 minutes. Nuclear counterstaining was performed using BOND Hematoxylin. The final immunohistochemical reaction was visualized by brown nuclear staining.
Subsequently, slides underwent dehydration and clearing through two immersions in Histanol 100, one mixed immersion in Histanol 100 and Bioclear, and three Bioclear immersions, each lasting 5 minutes. The procedure concluded with coverslipping using BMC-100 mounting medium.
Microscopic Evaluation. Positive expression of estrogen (anti-ER) and progesterone (anti-PR) receptors within intra- and peritumoral compartments was determined based on nuclear immunoreactivity. Immunopositivity was considered satisfactory when cells exhibited a clear nuclear pattern, highlighted by intense brown staining. Expression quantification was performed using the semi-automated protocol proposed by Pathology Outlines [24, 25].
Cell counting was conducted using an Olympus BX53 optical microscope equipped with an Olympus DP28 digital camera. ER+ and PR+ expression was quantitatively assessed in all cases, on a representative section from the paraffin block. Initially, at 100× magnification, areas of highest cellular expression ("hotspots") were identified, followed by quantification at 400× magnification.
Quantification methods. Quantification of ER-positive cells followed the semi-automated method described by Pathology Outlines [24, 25]. This approach involves assessing at least five microscopic fields at 40× objective magnification, selected from regions with the highest number of immunolabeled tumor cells, and calculating the mean percentage. To facilitate numeric evaluation, the tumor fields were photographed, and the images were contrast-inverted using Olympus cellSens Entry software.
Final assessment of ER and PR hormone marker expression was performed using the Allred scoring system, which combines the percentage of immunolabeled cells with the intensity of nuclear staining [26-28].
Ethical Considerations. Favorable approvals were obtained from the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy for two research projects: the first, titled “Molecular status of the tumor microenvironment in serous ovarian carcinoma,” approved by decision no. 8 on October 1, 2024; and the second, “Expression of growth and proliferation factors in high- and low-grade serous ovarian carcinoma,” approved by decision no. 2 on December 13, 2024.
Data analysis. Statistical analysis was performed using Winstat 2012.1 software (R. Fitch Software, Bad Krozingen, Germany), integrated into Microsoft Excel 2010, for preliminary descriptive and inferential data processing. To validate results and ensure comprehensive analysis, SPSS Statistics software version 23.0 (IBM, Chicago, IL, USA) was also employed.
Descriptive statistics included calculation of arithmetic mean (M), standard deviation (SD), and standard error of the mean (SE) for Allred scores of ER and PR hormone receptors, as well as for patients’ age distribution.
Comparison of quantitative variables between two groups – such as premenopausal versus postmenopausal patients – was performed using the Student's t-test for normally distributed data and the Mann–Whitney U test for non-parametric distributions. Differences among multiple groups (e.g., CA-125 levels stratified by FIGO stage and tumor grade) were evaluated using the Kruskal–Wallis test.
Correlations between hormone scores (Allred ER and PR) and clinicopathological parameters were examined using Spearman’s correlation coefficient (ρ). The association between ER/PR hormone profiles and FIGO stage distribution was assessed using the Chi-square test (χ²). All statistical analyses were interpreted at a significance level of p < 0.05.
Results
A retrospective analysis was performed on 40 cases of serous ovarian carcinoma, involving patients aged between 18 and 85 years. Age group distribution revealed a predominance in the 52-67 years range (42.5%) and the 35-51 years range (35%), with the majority of patients (75%) being postmenopausal.
Tumor localization was relatively evenly distributed, with 35% of cases involving the left ovary, 32.5% the right ovary, and 32.5% showing bilateral involvement. Histopathologically, 85% of the tumors were classified as high-grade serous carcinoma (HGSC), and 75% of patients were diagnosed at advanced stages according to the FIGO classification system (stage III-IV).
Estrogen receptor (ER) and progesterone receptor (PR) expression was evaluated using the Allred scoring system, which integrates the percentage of immunopositive cells with the staining intensity on a scale from 0 to 8 (Fig. 1 and 2).
ER expression was predominantly nuclear, with a diffuse pattern and variable intensity, yielding Allred scores ranging from 4 to 8 and an overall positivity rate of 60%. PR expression was more heterogeneous, with focal or mosaic patterns and weak to moderate intensity. The Allred scores for PR ranged from 2 to 6, with a total positivity rate of 50%.
a 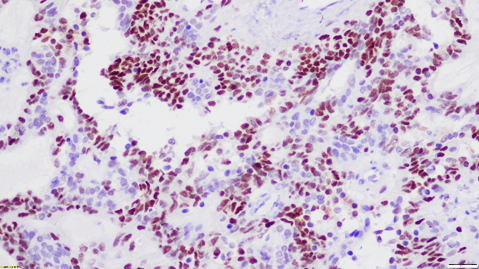 | b 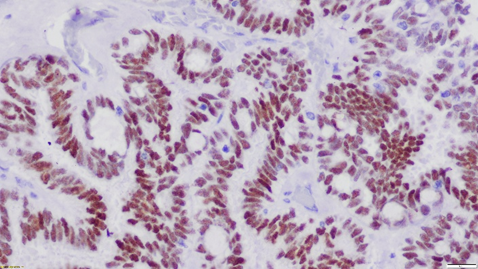 |
Fig. 1 Heterogeneous nuclear immunoexpression of estrogen receptor (ER) in serous ovarian carcinoma. (a) Low-magnification view (×20) showing patchy ER positivity within tumor cell nuclei. | |
a 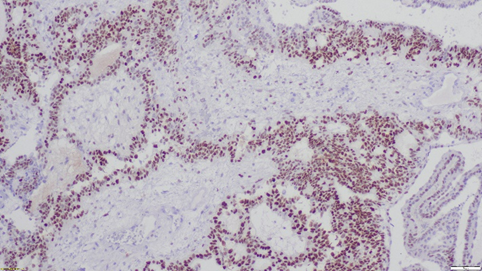 | b 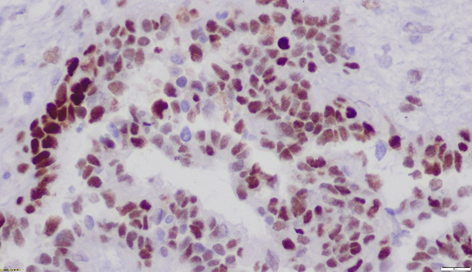 |
Fig. 2 Diffuse nuclear immunoexpression of progesterone receptor (PR) in serous ovarian carcinoma. Note: (a) Low-magnification view (×10) showing widespread nuclear positivity for PR in tumor cells. | |
Four immunohistochemical profiles were defined:
ER+/PR− – 25% of cases (10/40);
ER+/PR+ – 35% of cases (14/40);
ER−/PR+ – 15% of cases (6/40);
ER−/PR− – 25% of cases (10/40);
A moderate and statistically significant correlation was observed between Allred scores for ER and PR (ρ = 0.472, p = 0.001), indicating a partially synchronized hormonal expression pattern (Fig. 3).
The distribution of Allred ER and PR scores according to CA-125 categories revealed a statistically significant association (p = 0.001), with a predominance of positive hormone profiles (ER+/PR+) observed in cases with CA-125 levels ≤200 U/mL. In contrast, low PR scores were frequently associated with CA-125 levels >1000 U/mL, suggesting a more aggressive tumor biology.
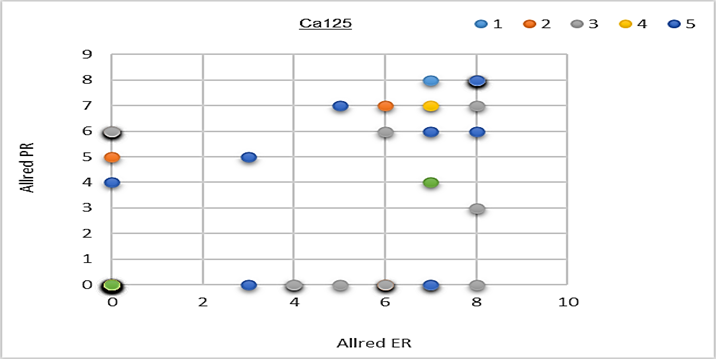 |  |
Fig. 3 Distribution of Allred ER and PR scores according to CA-125 levels Note: A statistically significant inverse relationship was noted between PR expression and CA-125 levels, with low PR scores predominating in tumors with CA-125 >1000 U/mL, suggesting a shift toward a more aggressive, hormone-resistant phenotype. | |
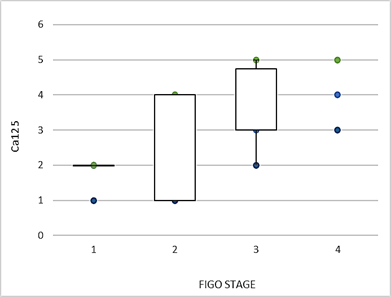 | 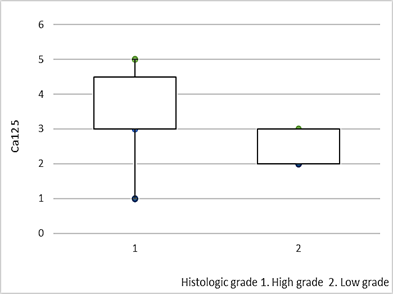 | 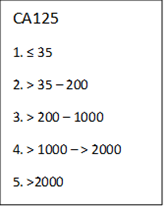 |
Fig. 4 Distribution of CA-125 levels according to FIGO stage and tumor grade, represented through comparative boxplots. Note: Higher CA-125 levels were significantly associated with advanced FIGO stages and high-grade serous carcinomas, supporting their role as surrogate markers of tumor aggressiveness. | ||
The Kruskal–Wallis test revealed statistically significant differences in the distribution of CA-125 levels both according to FIGO stage (H = 15.52, p = 0.0014) and tumor grade (H = 4.15, p = 0.041), with an ascending trend observed in serum marker levels among advanced stages and high-grade tumors (HGSC), suggesting prognostic relevance and an association with more aggressive tumor biology (Fig. 4).
The ER+/PR+ profile was predominant in patients with moderate CA-125 levels (≤200 U/mL), while profiles with reduced or absent PR expression (ER−/PR−) were frequently associated with elevated CA-125 levels (>1000 U/mL), suggesting a link between PR loss and tumor aggressiveness (Table 2).
Bilateral ovarian involvement was significantly associated with advanced FIGO stages (ρ = 0.657, p < 0.00001), highlighting the severity of neoplastic spread. Spearman correlation confirmed this association, indicating a clear trend toward tumor progression in cases with bilateral localization (ρ = 0.658, p < 0.00001), thus underscoring bilateral involvement as an unfavorable prognostic factor in serous ovarian carcinoma (Fig. 5).
Table 2. Distribution of patients according to ER/PR profile and serum CA-125 level | |||||
ER/PR profile vs CA125 | ≤35 | 36–200 | 201–1000 | 1001–2000 | >2000 |
ER+/PR+ | 1 | 2 | 6 | 3 | 2 |
ER+/PR− | 0 | 4 | 3 | 2 | 1 |
ER−/PR+ | 1 | 2 | 1 | 1 | 1 |
ER−/PR− | 0 | 1 | 5 | 3 | 1 |
Note: Positive ER/PR profiles were predominantly observed in patients with CA-125 levels ≤1000 U/mL, while double-negative (ER−/PR−) and ER−/PR+ phenotypes were more frequent at higher CA-125 levels, suggesting a potential link between hormonal receptor loss and elevated tumor burden. | |||||
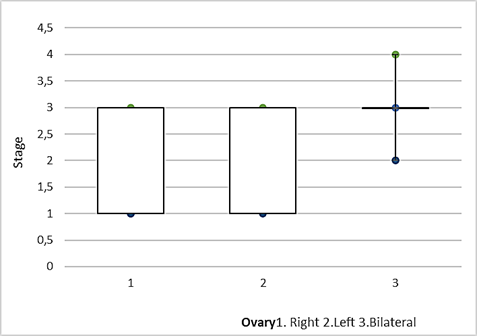 |
Fig. 5 FIGO stages according to ovarian localization (right, left, bilateral) – comparative boxplot. Note: Bilateral ovarian involvement was associated with significantly higher FIGO stages compared to unilateral cases, suggesting a more advanced tumor spread in bilaterally localized disease. |
Immunohistochemical profiles defined by Allred ER/PR scores demonstrated significant differences in FIGO stage distribution. The most advanced tumor extension was observed in the ER−/PR+ group (mean = 3.33), suggesting a possible association between the absence of estrogen receptor expression and disease severity (Fig. 6). Chi-square analysis confirmed a statistically significant association between hormone profiles and FIGO stage (χ² = 59.95, df = 39, p = 0.017). Comparison of Allred scores for hormone receptors between postmenopausal and premenopausal patients revealed no statistically significant differences. The analysis of Allred ER scores indicated a similar distribution of estrogen receptor expression across both groups (Z = 0.36, p = 0.719), while Allred PR scores showed a comparable profile of progesterone receptor expression (Z = 0.326, p = 0.745). These findings suggest that physiological hormonal status does not significantly influence ER and PR receptor expression levels in serous ovarian carcinoma (Fig. 7).
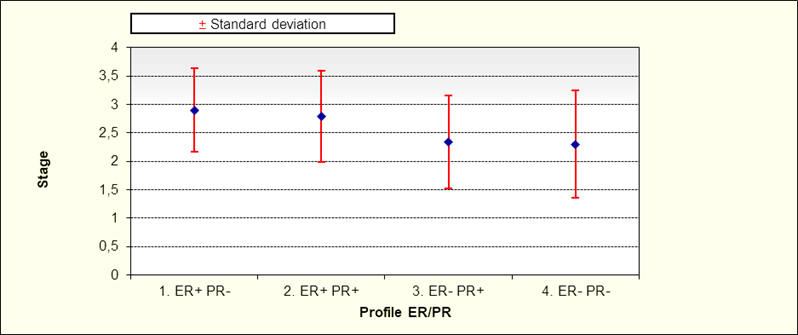 |
Fig. 6 Means and standard deviations of FIGO stage according to ER/PR hormonal profile Note: Lower FIGO stages were observed in ER+/PR+ tumors, while ER−/PR− profiles tended to associate with more advanced disease, supporting a link between hormone receptor negativity and tumor aggressiveness. |
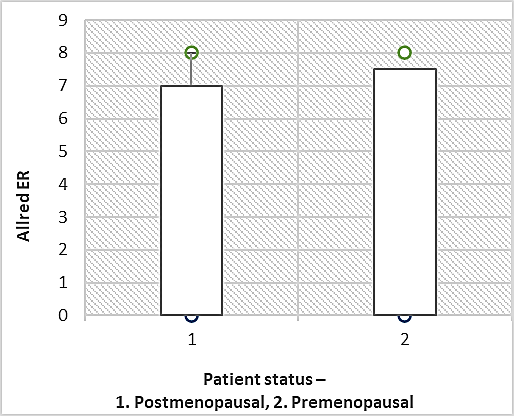 | 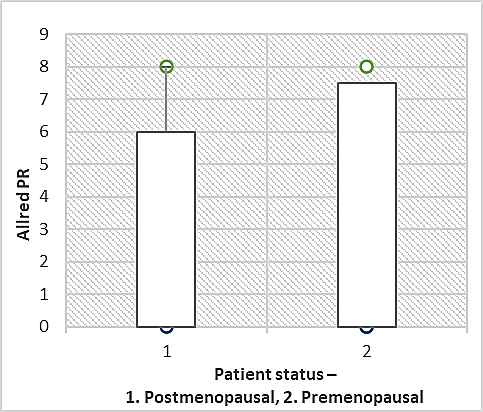 |
Fig. 7 Comparison of Allred ER and PR scores between postmenopausal and premenopausal patients Note: Premenopausal patients exhibited higher mean Allred scores for both ER and PR compared to postmenopausal counterparts, suggesting a more pronounced hormonal receptor expression profile in younger patients. | |
Discussion
The results obtained in this study suggest a significant relationship between hormone receptor expression and clinicopathological parameters in serous ovarian carcinoma. The moderate correlation observed between Allred scores for ER and PR reflects a partially synchronized hormonal profile, indicating that these receptors may hold complementary prognostic value in assessing tumor behavior. This finding is consistent with certain studies emphasizing the role of hormone receptors as relevant markers in various hormone-dependent neoplasms [29].
The differential distribution of hormonal scores in relation to CA-125 tumor marker levels revealed an association between reduced PR expression and elevated CA-125 values. This observation suggests a more aggressive tumor biology and a potential loss of the protective influence of PR in serous ovarian carcinoma, a concept supported by previous data linking lower PR levels with poorer prognosis [29]. Additionally, significant differences in CA-125 levels based on FIGO stage and tumor grade reaffirm the prognostic importance of this marker, with higher values characteristic of advanced stages and high-grade serous carcinoma (HGSC), reflecting greater disease extent and aggressiveness [30, 31].
The association between bilateral ovarian involvement and advanced stages of disease supports the hypothesis that bilateral extension indicates a more aggressive and unfavorable prognostic profile. This finding underscores the importance of evaluating bilaterality in morphopathological examination as a complementary prognostic factor [30, 31].
Chi-square analysis revealed a statistically significant association between ER/PR hormonal profiles and tumor extension stage, with an increased prevalence of advanced disease observed in the ER−/PR+ group. This suggests that the absence of estrogen receptor expression, coupled with progesterone receptor positivity, may represent a distinct biological phenotype with implications in neoplastic progression [32]. This observation opens avenues for future research exploring the molecular mechanisms underpinning these phenotypes and assessing their potential as therapeutic targets or specific prognostic markers.
Although comparative analysis of hormone receptor expression between postmenopausal and premenopausal patients did not yield significant differences, this finding should be interpreted with caution, considering the relatively small sample size and potential confounding variables that could not be fully controlled in this study [18, 33]. Physiological hormonal changes are known to influence receptor expression, but their relevance in the context of serous ovarian carcinoma requires further investigation in larger cohorts with detailed hormonal status analysis.
Major limitations of the study include the relatively small cohort size, which may affect statistical power and the generalizability of results. Additionally, the absence of detailed molecular data – such as BRCA mutational status or extended genomic profiling – represents an important gap that may influence both hormone receptor expression and patient prognosis. Integrating these molecular insights could provide a deeper understanding of the biological heterogeneity of serous ovarian carcinoma and facilitate the development of personalized therapeutic strategies based on individual tumor characteristics.
Conclusions
The data obtained in this study support the hypothesis that estrogen (ER) and progesterone (PR) hormone receptor expression has clinically and prognostically relevant significance in serous ovarian carcinoma, significantly influencing clinicopathological parameters and tumor behavior. In particular, the correlations identified between receptor expression and CA-125 tumor marker levels, as well as with disease progression stage, highlight the important role of ER and PR in defining the tumor’s biological profile. Hormonal profiles established using the Allred scoring system provide valuable prognostic insights, and the association between low PR expression and more aggressive tumor forms reveals the potential of this marker as an indicator of disease severity. Additionally, the correlation between bilateral ovarian involvement and advanced cancer stages underscores the importance of morphopathological parameters in prognostic stratification. However, to validate and further explore these findings, additional studies are required, incorporating larger cohorts and detailed molecular analyses, thereby facilitating the development of optimized therapeutic strategies tailored to the tumor’s molecular profile.
Competing interests
None declared.
Authors’ contributions
VP conceived the study, contributed to the design and case selection, participated in data analysis, and drafted the initial version of the manuscript. TM carried out the histopathological evaluation of all cases, conducted detailed microscopic analyses, and was responsible for the quantification of immunopositive cells, playing a crucial role in ensuring the accuracy of the morphological assessment. VD performed all laboratory procedures, including immunohistochemical staining, protocol optimization, and preparation of histological sections. EF contributed to the histological interpretation and provided partial supervision of the scientific content of the project. LȘ served as the scientific coordinator of the study, critically contributed to data interpretation, ensured scientific validation, and participated in drawing the final conclusions. All authors were involved in the writing and revision of the manuscript, critically reviewed the content, and approved the final version of the article.
Acknowledgements and funding
The authors express their sincere gratitude to the staff of the Laboratory of Morphology at Nicolae Testemițanu State University of Medicine and Pharmacy for their valuable technical assistance in specimen processing. The authors also acknowledge the support provided by the Institute of Oncology and the Department of Histology, Cytology, and Embryology of Nicolae Testemițanu State University of Medicine and Pharmacy for their institutional collaboration throughout the course of the study.
Ethics approval
Favorable approvals were obtained from the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy for two research projects: “Molecular status of the tumor microenvironment in serous ovarian carcinoma,” approved by decision no. 8 on October 1, 2024; and the second, “Expression of growth and proliferation factors in high- and low-grade serous ovarian carcinoma,” approved by decision no. 2 on December 13, 2024.
Provenance and peer review
Not commissioned, externally peer reviewed.
Authors’ ORCID IDs
Valeria Pînzaru – https://orcid.org/0009-0000-8834-7743
Tatiana Mărițoi – https://orcid.org/0009-0007-6861-557X
Valeriu David – https://orcid.org/0000-0001-9799-7369
Ecaterina Foca – https://orcid.org/0000-0001-7629-4875
Lilian Șaptefrați – https://orcid.org/0000-0003-2779-718X
References
Fumagalli D, Jayraj A, Olearo E, Capasso I, Hsu HC, Tzur Y, et al. Primary versus interval cytoreductive surgery in patients with rare epithelial or non-epithelial ovarian cancer. Int J Gynecol Cancer. 2025;35(3):101664. doi: 10.1016/j.ijgc.2025.101664.
Ledermann JA, Matias-Guiu X, Amant F, Concin N, Davidson B, Fotopoulou C, et al. ESGO–ESMO–ESP consensus conference recommendations on ovarian cancer: pathology and molecular biology and early, advanced and recurrent disease. Ann Oncol. 2024;35(3):248-66. doi: 10.1016/j.annonc.2023.11.015.
World Cancer Research Fund International. Ovarian cancer statistics [Internet]. London: The Fund; c2025- [cited 2025 May 16]. Available from: https://www.wcrf.org/preventing-cancer/cancer-statistics/ovarian-cancer…
National Cancer Institute (US). Cancer stat facts: ovarian cancer [Internet]. Bethesda: SEER; 2025 [cited 2025 May 16]. Available from: https://seer.cancer.gov/statfacts/html/ovary.html
Matulonis UA, Sood AK, Fallowfield L, Howitt BE, Sehouli J, Karlan BY. Ovarian cancer. Nat Rev Dis Primers. 2016;2:16061. doi: 10.1038/nrdp.2016.61.
Wei YF, Ning L, Xu YL, Ma J, Li DR, Feng ZF, et al. Worldwide patterns and trends in ovarian cancer incidence by histological subtype: a population based analysis from 1988 to 2017. eClinicalMedicine. 2024;79:102983. doi: 10.1016/j.eclinm.2024.102983.
World Health Organization, International Agency for Research on Cancer (IARC). WHO classification of tumours: Female genital tumours. 5th ed. Lyon (France): IARC; 2020. 635 p.
Devouassoux Shisheboran M, Genestie C. Pathobiology of ovarian carcinomas. Chin J Cancer. 2015;34(1):50-5. doi: 10.5732/cjc.014.10273.
Babaiier A, Mal H, Alselwi W, Ghatage P. Low grade serous carcinoma of the ovary: the current status. Diagnostics (Basel). 2022;12(2):458. doi: 10.3390/diagnostics12020458.
Cappuccio S, Marchetti C, Altıntaş DA, Oliva R, Russo SA, Costantini B, et al. Low-grade versus high-grade serous ovarian cancer: comparison of surgical outcomes after secondary cytoreductive surgery. Int J Gynecol Cancer. 2024;34(2):293-9. doi: 10.1136/ijgc-2023-004854.
Köbel M, Kang EY. The evolution of ovarian carcinoma subclassification. Cancers (Basel). 2022;14(2):416. doi: 10.3390/cancers14020416.
Smolarz B, Biernacka K, Łukasiewicz H, Samulak D, Piekarska E, Romanowicz H, et al. Ovarian cancer – epidemiology, classification, pathogenesis, treatment, and estrogen receptors’ molecular backgrounds. Int J Mol Sci. 2025;26(10):4611. doi: 10.3390/ijms26104611.
Barili V, Ambrosini E, Bortesi B, Minari R, De Sensi E, Cannizzaro IR, et al. Genetic basis of breast and ovarian cancer: approaches and lessons learned from three decades of inherited predisposition testing. Genes (Basel). 2024;15(2):219. doi: 10.3390/genes15020219.
Gambini D, Ferrero S, Kuhn E. Lynch syndrome: from carcinogenesis to prevention interventions. Cancers (Basel). 2022;14(17):4102. doi: 10.3390/cancers14174102.
Schüler Toprak S, Weber F, Skrzypczak M, Ortmann O, Treeck O. Expression of estrogen related receptors in ovarian cancer and impact on survival. J Cancer Res Clin Oncol. 2021;147(8):2555-67. doi: 10.1007/s00432-021-03673-9.
Zhang M, Xu H, Zhang Y, Li Z, Meng W, Xia J, et al. Research progress of estrogen receptor in ovarian cancer. Clin Exp Obstet Gynecol. 2023;50(1):199. doi: 10.31083/j.ceog5009199.
Borella F, Fucina S, Mangherini L, Cosma S, Carosso AR, Cusato J, et al. Hormone receptors and epithelial ovarian cancer: recent advances in biology and treatment options. Biomedicines. 2023;11(8):2157. doi: 10.3390/biomedicines11082157.
Tan J, Song C, Wang D, Hu Y, Liu D, Ma D, Gao Q. Expression of hormone receptors predicts survival and platinum sensitivity of high grade serous ovarian cancer. Biosci Rep. 2021;41(5):BSR20210478. doi: 10.1042/BSR20210478.
Aubert M, Mathiot L, Vegas H, Ouldamer L, Linassier C, Augereau P, et al. Endocrine therapy in advanced high-grade ovarian cancer: real-life data from a multicenter study and a review of the literature. Oncologist. 2024;29(7):e910-e917. doi: 10.1093/oncolo/oyae093.
Harbeck N, Penault-Llorca F, Cortes J, Gnant M, Houssami N, Poortmans P, et al. Breast cancer. Nat Rev Dis Primers. 2019;5(1):66. doi: 10.1038/s41572-019-0111-2.
Early Breast Cancer Trialists' Collaborative Group (EBCTCG); Davies C, Godwin J, Gray R, et al. Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomised trials. Lancet. 2011;378(9793):771-84. doi: 10.1016/S0140-6736(11)60993-8.
Llaurado Fernandez M, Dawson A, Kim H, Lam N, Russell H, Bruce M, et al. Hormone receptor expression and outcomes in low-grade serous ovarian carcinoma. Gynecol Oncol. 2020;157(1):12-20. doi: 10.1016/j.ygyno.2019.11.029.
Lin TH, Gao HW, Liao GS, Yu JC, Dai MS, Ho JY, et al. Amongst women stratified to receive endocrine therapy on the basis of their tumor estrogen and progesterone receptor levels, those with higher tumor progesterone receptor levels had a better outcome than those with lower levels of tumor progesterone receptor. Cancers (Basel). 2021;13(4):905. doi: 10.3390/cancers13040905.
Haghi L, Jorns JM. Estrogen receptor. 2024 Aug 1. In: PathologyOutlines.com [Internet]. Michigan: PathologyOutlines.com; c2002-2025 [cited 2025 May 23]. Available from: https://www.pathologyoutlines.com/topic/stainser.html
Huether S, Jorns JM. Progesterone receptor (PR). 2024 Jul 29. In: PathologyOutlines.com [Internet]. Michigan: PathologyOutlines.com; c2002-2025 [cited 2025 May 23]. Available from: https://www.pathologyoutlines.com/topic/stainsprog.html
Allred DC, Harvey JM, Berardo M, Clark GM. Prognostic and predictive factors in breast cancer by immunohistochemical analysis. Mod Pathol. 1998;11(2):155-68.
Suneja P, Saldanha P. Histopathological study of endometrium in abnormal uterine bleeding with expression of oestrogen and progesterone receptors. New Indian J Obstet Gynecol. 2024;10(2):274-280. doi: 10.21276/obgyn.2024.10.2.7.
Öztürk Ç, Okcu O, Öztürk SD, Şen B, Öztürk AE, Bedir R. Reporting hormone receptor expression in breast carcinomas: which method has the highest prognostic power and what should be the optimal cut-off value? Int J Surg Pathol. 2025;33(2):353-62. doi: 10.1177/10668969241265068.
Gupta D, Lis CG. Role of CA125 in predicting ovarian cancer survival - a review of the epidemiological literature. J Ovarian Res. 2009;2:13. doi: 10.1186/1757-2215-2-13.
Wang Q, Feng X, Liu X, Zhu S. Prognostic value of elevated pre-treatment serum CA-125 in epithelial ovarian cancer: a meta-analysis. Front Oncol. 2022;12:868061. doi: 10.3389/fonc.2022.868061.
Charkhchi P, Cybulski C, Gronwald J, Wong FO, Narod SA, Akbari MR. CA125 and ovarian cancer: a comprehensive review. Cancers (Basel). 2020;12(12):3730. doi: 10.3390/cancers12123730.
Ng CW, Wong KK. Impact of estrogen receptor expression on prognosis of ovarian cancer according to antibody clone used for immunohistochemistry: a meta-analysis. J Ovarian Res. 2022;15(1):63. doi: 10.1186/s13048-022-01001-4.
Gupta S, Ahuja S, Kalwaniya DS. Immunohistochemistry markers in ovarian and fallopian tube neoplasms: a comprehensive review. Indian J Surg Oncol. 2024;15(Suppl 3):465-80. doi: 10.1007/s13193-024-02049-y.