

Introduction
The common carotid artery (CCA) is the main source of blood supply to the head and neck regions. At the superior border of the thyroid cartilage, it bifurcates into its primary branches: the internal carotid artery (ICA) and the external carotid artery (ECA). However, anatomical and imaging studies have revealed significant variability in the origin, level and angle of its bifurcation and branching patterns of the CCA [1-3].
Disturbances of the embryonic development at any Carnegie stage can result in abnormal development of the arterial system components, which can be caused by the regression or disappearance of some blood vessels, or due to their incomplete development [4]. In cases of arterial variants, they are detected during routine examinations by imaging methods or postmortem by anatomical dissection [5, 6].
According to bibliographic sources, about 10% of malpractice was recorded in surgical patients with anatomical variants [5]. The contemporary methods of imaging such as computed tomography, nuclear magnetic resonance, and three-dimensional reconstructions, offer the possibility of preoperative visualization of the blood vessels, decreasing the rate of iatrogenic injures [7].
Among the clinically important, anatomical branching pattern variants of CCA, is the origin of the superior thyroid artery directly from the common carotid artery, or its deviation from the main trunk of the CCA at the level of its bifurcation, with a variation rate of 2.2% - 61% [1, 8-10].
According to the results obtained by Esen et al. in 2018, who performed a large study on 1280 angiographies, the origin of the right superior thyroid artery from the CCA bifurcation was found in 20.5% of cases and of the left artery in 23.1% [11]. The origin of the superior thyroid artery directly from the CCA was reported in 14.1% of cases on the right and 35.3% on the left, respectively.
Bhardwaj et al. analyzed the origin of the superior thyroid artery on a sample size of 210 subjects [12]. The obtained result showed that in 14.3% of cases the superior thyroid artery derived at the level of the CCA bifurcation, while in 8.6% it originated directly from the CCA trunk.
The variability of the superior thyroid artery origin and its relationships to the superior laryngeal nerve are of particular importance in thyroidectomy [13]. In surgical interventions on the thyroid gland, injuries to the superior laryngeal nerve can occur at rates as high as 58% [14, 15].
Quadri- and pentafurcation of the CCA have been reported in the specialized literature as rare anatomical variants. Zaccheo et al. described a rare case of pentafurcation in which the CCA divided into the superior thyroid artery, lingual artery, facial artery, external carotid artery and internal carotid artery [16]. Kaneko et al. described another very rare case, when the superior thyroid artery, lingual artery and facial artery derived directly from the CCA, while the posterior auricular, maxillary and superficial temporal arteries arose from a common trunk. The internal carotid artery also originated from the CCA, and the occipital and ascending pharyngeal arteries arose from it [17].
Knowledge of anatomical variants related to CCA branching patterns is important both an anatomical and a clinical perspective. These variations can influence the planning of vascular, endovascular and oncological interventions in the head and neck regions, and are extremely important for avoiding vascular injuries and improving intraoperative and postoperative management [13, 18].
The purpose of our study was to identify anatomical variations in the CCA branching patterns depending on gender and laterality.
Material and methods
Variants of the CCA branching patterns were studied retrospectively on a sample size of 210 patients who underwent CT angiography of the carotid artery during the period 2020-2024, at the Institute of Emergency Medicine and the Republican Center for Medical Diagnostics. The study was approved by the Research Ethics Committee of Nicolae Testemitanu State University of Medicine and Pharmacy, based on decision No.3 dated 27.01.2025. The representative sample size was calculated using the EpiInfo7.2.2.6 program, under the “StatCalc – Sample Size and Power” module, based on the following parameters: confidence interval – 95.0% for statistical significance, statistical power – 80.0%, an expected outcome difference of 20.0% in patients with anatomical variants of the common carotid artery, PR = 2, and an equal group ratio of 1:1. The calculated value was 182, after adjusting for an estimated non-response rate of 10.0%, the final required sample size was 200.
The study group included 118 males and 92 females. The mean age of male patients was 63.6±13.44 years and the mean age of female patients was 65.1±14.32 years, (p = 0.444). To achieve the proposed aim and objectives, angiographic images of 400 carotid arteries were analyzed and processed. Based on this analysis, the absolute and relative values of the incidence of common carotid artery branching patterns were determined, depending on sex, laterality and neighboring anatomical landmarks. For CT angiographies of the carotid artery, the Canon Aquilion 320 slices computed tomography, which provides high-resolution images, was used. Subsequently, the angio-CT images were analyzed and interpreted using the RadiAnt DICOM Viewer 2024.1 software, with capacity of multiplanar and three-dimensional reconstructions and maximum intensity projections, which allowed us to visualize in detail the branching variants of the CCA and to perform their morphometry. The data were stored in an Excel database, and statistical analysis was performed using predefined statistical functions in Excel. The frequency of anatomical variants according to sex, laterality, and neighboring anatomical landmarks was estimated by calculating the confidence interval at a 95% confidence interval.
To enhance the accuracy of the study, clear inclusion and exclusion criteria were established, allowing for the selection of a representative and homogeneous group of participants.
Inclusion criteria:
Patients examined by CT angiography of the carotid artery >18 years old;
Patients with clear and visible angiographic images.
Exclusion criteria:
Patients examined by CT angiography of the carotid artery <18 years old;
Patients with unclear or poor-quality angiographic images;
Patients who have undergone surgical interventions involving the carotid arteries;
Patients in flexion, retroflexion or laterally tilted head.
Results
In the current study, 420 CCAs were examined. The most frequent branching pattern of the CCA, considered a normal variant, was its bifurcation into ICA and ECA, being identified on the right side in 70% of cases (n = 147) and on the left side in 54% (n = 113). This variant was more frequently found in males (55.3%).
Another branching pattern variant of the CCA was its trifurcation into the ICA, ECA and superior thyroid artery (Fig. 1). The CCA trifurcation was more prevalent on the left side (33.3%) than on the right side (25.7%). The bilateral distribution of the CCA trifurcation was observed in 16.9% (n = 21), predominating in males (57.1%), compared to females (42.8%).
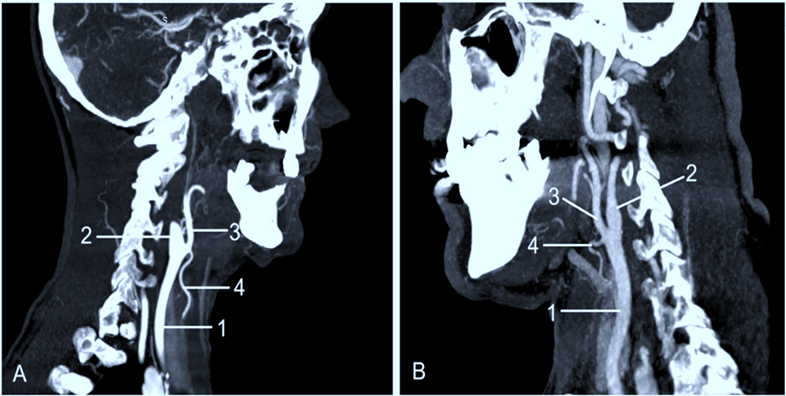 |
Fig. 1 Trifurcation of the common carotid artery. A. Lateral view (right side). B. Lateral view (left side). 1 – common carotid artery; 2 – internal carotid artery; 3 – external carotid artery; 4 – superior thyroid artery. |
On the right side, the trifurcation of the CCA was found in 57.4% of males (n = 31), while in females, the rate was 42.5% (n = 23). The left CCA trifurcation was found in 55.7% (n = 39) of males, and in 44.2% (n = 31). Our results showed a slight bilateral predominance of CCA trifurcation in males. The distribution of this variant depending on gender and laterality is presented in figure 2.
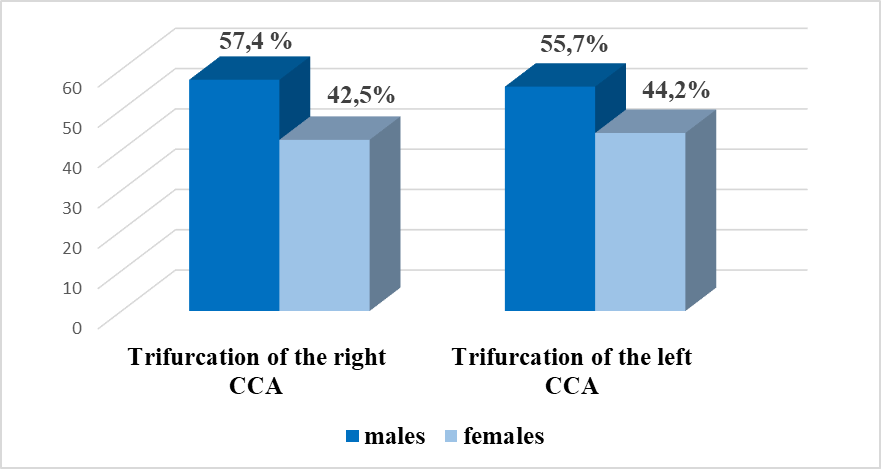 |
Fig. 2 Sex-based distribution of the common carotid trifurcation Note: CCA – common carotid artery |
In 16.6% of cases, the common carotid artery divided into three branches ICA, ECA and superior thyroid artery (STA). The STA originated directly from the CCA below its bifurcation (Fig. 3). This variant was observed on the right side in 12.8% of cases and on the left side in 3.8%.
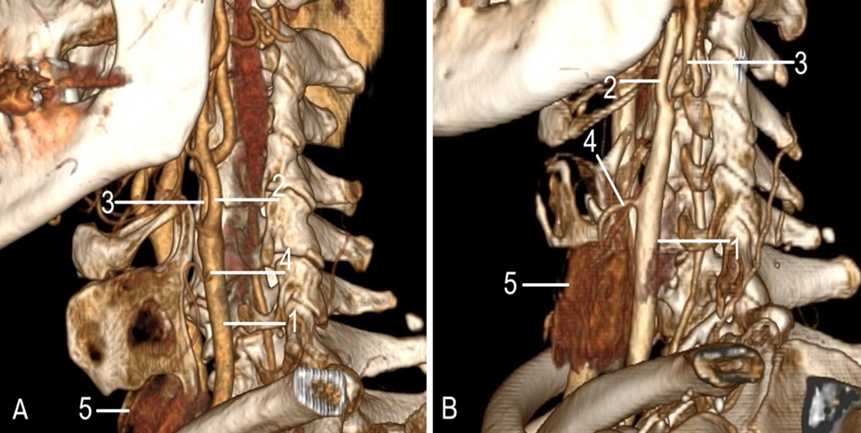 |
Fig. 3 Origin of the superior thyroid artery directly from the common carotid artery. A, B. Anterolateral view (left side). 1 – common carotid artery; 2 – external carotid artery; 3 – internal carotid artery; 4 – superior thyroid artery; 5 – thyroid gland. |
Similar to the CCA trifurcation, this variant (a high-origin superior thyroid artery) was more prevalent in males. In the male cohort, its distribution was nearly equal bilaterally, occurring on the right side in 62.5% of cases and on the left in 62.6%.In females, the distribution was also nearly equal between the left and right sides (37.5% and 37.0%, respectively).. The bilateral distribution of the origin of the superior thyroid artery below the bifurcation level per study group reached a rate of 11.4%.
As a result of the morphometry of the distance between the CCA bifurcation (CCAB) and the origin of the superior thyroid artery (OSTA), four groups of variables were established (Fig.4).
Group I included patients with the distance between OSTA and CCAB < 0.5 cm;
Group II – patients with the distance between OSTA and CCAB 0.51 cm – 1 cm;
Group III – patients with the distance between OSTA and CCAB 1.1 cm – 1.5 cm;
Group IV – patients with the distance between OSTA and CCAB > 1.51 cm.
The obtained results demonstrate a higher frequency of the origin of the superior thyroid artery at a distance < 0.5 cm in relation to the level of the CCA bifurcation. This proximity may create uncertainty when identifying the STA during surgical interventions on the thyroid gland.
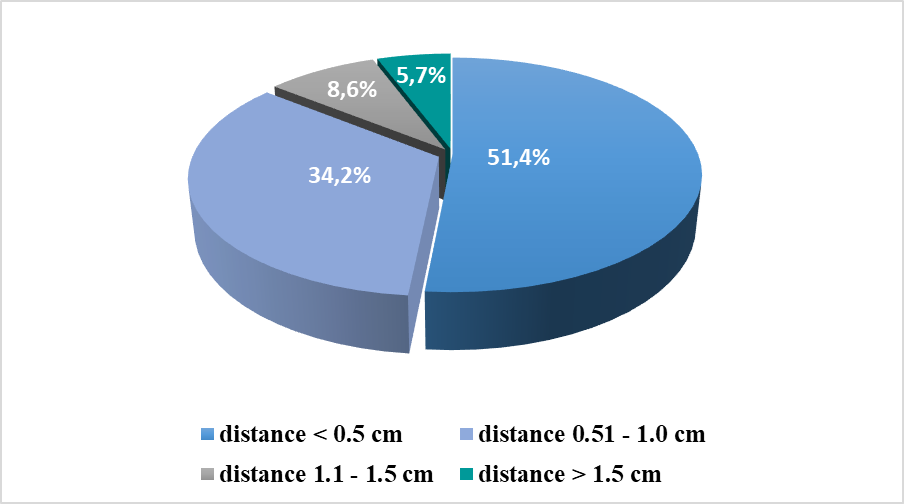 |
Fig. 4 Range-based analysis of superior thyroid artery origin relative to the common carotid artery bifurcation. |
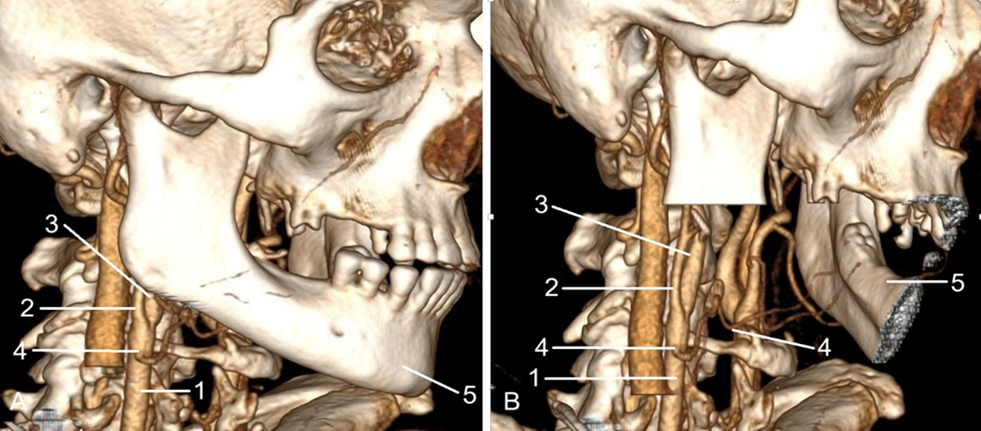
The origin of the superior thyroid artery from the level of the CCA bifurcation and directly from its trunk was analyzed in relation to the greater horn of the hyoid bone, which is an important anatomical landmark in the cervical region (Fig. 5).
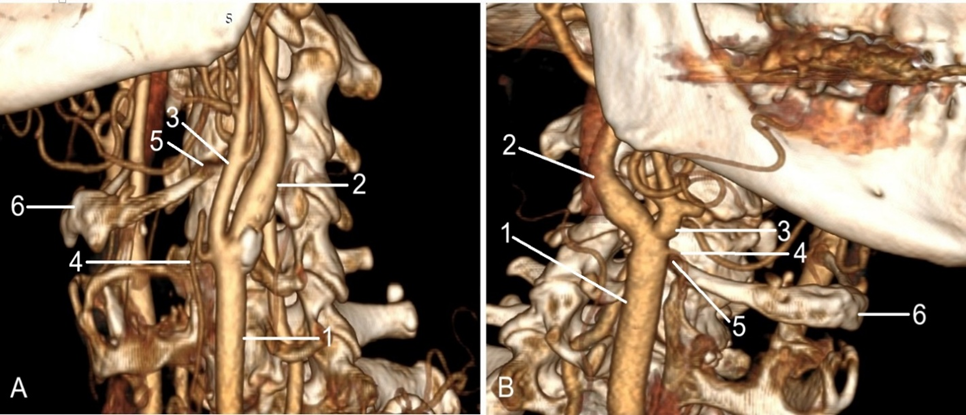 |
Fig. 5 Origin of the superior thyroid artery in relation to the hyoid bone. A. Anterolateral view (left side). Origin of the superior thyroid artery, below the hyoid bone. B. Anterolateral view (right side). Origin of the superior thyroid artery, above the hyoid bone. 1 – common carotid artery; 2 – internal carotid artery; 3 – external carotid artery; 4 – superior thyroid artery; 5 – greater horn of the hyoid bone |
Our results showed that in 20.1% of cases, the origin of the STA was above the greater horn of the hyoid bone, and in 14.5% of cases, it was at the level of the greater horn of the hyoid bone, and in 65.4% of cases it was below it.
When analyzed by laterality, the most common location for the superior thyroid artery’s origin was below the greater horn of the hyoid bone. This pattern was observed in 64.5% of cases on the right side and 66.0% on the left. On the left side, the artery originated superior to the greater horn in 21.6% of cases and at the same level as the horn in 12.3%. On the right side, the artery's origin was superior to the horn in 17.7% of cases and at the same level as the horn in another 17.7%. Among the anatomical variants highlighted in the study group, a rare branching pattern of the CCA, from which derived the ICA, ECA and lingual artery was identified (Fig. 6).
|
Fig. 6 Origin of the lingual artery directly from the common carotid artery. A, B. anterolateral view, right side. 1 – common carotid artery; 2 – external carotid artery; 3 – internal carotid artery; 4 – superior thyroid artery. |
This variant was detected in a single female patient, constituting 0.4%. In this case, the lingual artery originated directly from the lateral semicircumference of the CCA, 0.91 cm below the main bifurcation. The artery then followed a semi-arcuate path, oriented anteromedially to the CCA, before continuing toward the tongue.
Discussion
According to bibliographic sources, there is evidence of increased variability of the common carotid artery branching patterns [2, 8, 15, 18, 19]. The most common variant, considered a normal variant, is the bifurcation of the common carotid artery into the internal carotid artery and the external carotid artery, reported in 61.5% [19]. In our study, the bifurcation of the CCA was found in 70% of cases on the right side and in 54% on the left side.
Other anatomical variants described in the specialty literature are the trifurcation, quadrifurcation and pentafurcation of the CCA. Ogeng's et al. conducted a study on 208 cadavers, reporting trifurcation of the CCA into the ICA, ECA and superior thyroid artery in 31.7% of cases [19]. Quadrifurcation of the CCA into the ICA, ECA, superior thyroid artery and ascending pharyngeal artery was found in 5.4%, and pentafurcation of the CCA into the ICA, ECA, superior thyroid artery, posterior auricular artery and occipital artery was revealed in 1.4%.
Some authors pointed out that CCA trifurcation, when the third branch is the superior thyroid artery, is the most common variant. Gupta et al. reported this variant in 21.5% of cases on the right side and 18.5% on the left [20], while Vazquez et al. observed a twice higher frequency of that variant, up to 49% [21].
Our results are in line with the data reported in the literature, but with a slight predominance of trifurcation on the left side with a ratio left/right of 33.3%/25.7%. Quadrifurcation and pentafurcation of the CCA were not identified in our sample size.
The direct origin of the superior thyroid artery from the CCA trunk, or from its bifurcation level has been studied by several authors. Calotă et al. found direct origin of the STA from the CCA in 8.8% and from the level of the CCA bifurcation in 28.8% [22]. Poutoglidis et al. conducted a meta-analysis study of the superior thyroid artery origin on 5488 cases, reported in the literature [23]. Their results showed that in 55% of cases the superior thyroid artery derived from the ECA. The STA origin from the level of the CCA bifurcation was marked out in 27.5%, from the CCA trunk in 15% and, very rarely, from the ICA with a rate of 0.05%, while Herrera-Núñez et al. found the origin of the superior thyroid artery at the CCA bifurcation in 20.4% of cases, and the direct from the CCA was reported in 17.1% [24].
In our study, the origin of the superior thyroid artery from the bifurcation level of the CCA was observed in 29.5% and in 8.3% from its trunk. Our results are consistent with data reported in the literature.
Knowledge about the origin of the superior thyroid artery is essential in planning surgical interventions. According to Tzortziset et al. in thyroid surgery, the superior thyroid artery should be ligated as close as possible to its origin, to avoid injury to the superior laryngeal nerve [25].
The origin of the superior thyroid artery from the CCA trunk, or from its bifurcation has been studied in relation to the hyoid bone. Calotă et al. classified the detected variants into three groups: infrahyoid origin (47%), origin at the level of the greater horn of the hyoid bone (25.8%), and suprahyoid origin (24.7%) [22].
Our data demonstrated the prevalence of the origin of the superior thyroid artery inferior to the greater horn of the hyoid bone in 65.4%. The suprahyoid origin was identified in 20.1% of cases, and its origin at the level of the greater horn of the hyoid bone was found in 14.5%.
The direct origin of the thyrolingual trunk from the CCA represents a rare variant of the CCA branching pattern, with a rate of 0.3%-1% [26]. Kapre et al. reported a case of the thyrolingual trunk origin from the level of the CCA bifurcation and in another case, the thyrolingual trunk was noted at 17 mm below the CCA bifurcation [27].
In rare cases the lingual artery derives directly from the CCA. Jadhov et al. reported a clinical case, when the lingual artery originated from the medial circumference of the CCA, at 6 mm below the CCA bifurcation [28].
Our results confirmed the data reported in the specialty literature, thus, in 0.4% of cases, the lingual artery derived directly from the CCA, at 9.1 mm below its bifurcation.
Conclusions
Knowledge of the common carotid artery branching pattern variation and its topographic relationships with the neighboring anatomical landmarks is of high clinical significance, playing an essential role in preventing intraoperative complications and improving the quality of surgical management.
Competing interests
None declared.
Authors’ contributions
Conception and design of the work – NO, AB, IC. Contribution to acquisition of data NO. Contribution to analysis and interpretation of data NO, AB. Drafting the article NO, AB, IC, AB, ZZ. All authors critically reviewed the work and approved the final version of the manuscript.
Ethics approval
The research project was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (Minutes no. 3 from 27.01.2025).
Patient consent
Obtained.
Acknowledgements and funding
No external funding.
Provenance and peer review
Not commissioned, externally peer reviewed.
Authors’ ORCID IDs
Nadia Ostahi – https://orcid.org/0009-0003-7197-0178
Angela Babuci – https://orcid.org/0000-0003-0305-1279
Ilia Catereniuc – https://orcid.org/0000-0002-5479-4198,
Anastasia Bendelic – https://orcid.org/0000-0002-2838-3168
Zinovia Zorina – https://orcid.org/0000-0002-0749-6083
References
1. Biskupski M, Homzar S, Dąbrowska Z, Buczek J, Daniluk A, Iwaniuk K, et al. Clinical implications of variations of common carotid artery trifurcation. J Pre Clin Clin Res. 2024;18(1):83-7. https://doi.org/10.26444/jpccr/186029.
2. Abdalla M, Mohammed N, Abdallah R, Ahmed MK, Abdelrahim M, Salih A, et al. Anatomical variations of the bifurcation levels of the common carotid artery and superior thyroid artery. Cureus. 2024;16(10):e71120. doi: 10.7759/cureus.71120.
3. Kumar M, Kumar A, Ahuja CK, Khurana D. (Un)common carotid trifurcation. Neurol India. 2025;73(2):349-351. doi: 10.4103/neuroindia.NI_370_19.
4. Zorina Z, Catereniuc I, Babuci A, Botnari T, Certan G. Variants of branching of the upper limb arteries. Mold Med J. 2017;60(4):33-38. doi: 10.5281/zenodo.1106127.
5. Alraddadi A. Literature review of anatomical variations: clinical significance, identification approach, and teaching strategies. Cureus. 2021;13(4):e14451. doi: 10.7759/cureus.14451.
6. Rodriguez A, Cobeñas R, Gallo JC, Salamida A, Larrañaga N, Kozima S. Variantes anatómicas vasculares halladas de manera incidental en estudios de tomografía computada [Incidental findings of vascular anatomic variants on computed tomography]. Rev Argent Radiol. 2013;77(1):19-25. Spanish. doi: 10.7811/rarv77n1a03.
7. Sharma R, Nishan S, Yadav SK, Choudhary D. A comprehensive review of anatomical variations and their clinical significance in surgical procedures . J Ayurveda Integr Med Sci. 2025;10(5). https://doi.org/10.21760/jaims.10.5.20.
8. Thenmozhi A, Subadha C, Aruna K, Prabavathi P. Variations in the origin of superior thyroid artery-a cadaveric study in the south indian population. Int J Acad Med Pharm, 2024;6(4):526-529. doi: 10.47009/jamp.2024.6.4.103.
9. Triantafyllou G, Paschopoulos I, Duparc F, Tsakotos G, Tsiouris C, Olewnik Ł, Georgiev G, Zielinska N, Piagkou M. The superior thyroid artery origin pattern: a systematic review with meta-analysis. Surg Radiol Anat. 2024;46(9):1549-1560. doi: 10.1007/s00276-024-03438-2.
10. Borges A, Ramalho S, Ferreira L. Common carotid artery trifurcation: a potentially dangerous anatomical variant. BMJ Case Rep. 2021;14(2):e241104. doi: 10.1136/bcr-2020-241104.
11. Esen K, Ozgur A, Balci Y, Tok S, Kara E. Variations in the origins of the thyroid arteries on CT angiography. Jpn J Radiol. 2018;36(2):96-102. doi: 10.1007/s11604-017-0710-3.
12. Bhardwaj Y, Singh B, Bhadoria P, Malhotra R, Tarafdar S, Bisht K. Computed tomography angiographic study of surgical anatomy of thyroid arteries: clinical implications in neck dissection. World J Radiol. 2023;15(6):182-190. doi: 10.4329/wjr.v15.i6.182.
13. Dessie MA. Variations of the origin of superior thyroid artery and its relationship with the external branch of superior laryngeal nerve. PLoS One. 2018;13(5):e0197075. https://doi.org/10.1371/journal.pone.0197075.
14. Kowalczyk KA, Majewski A. Analysis of surgical errors associated with anatomical variations clinically relevant in general surgery. Review of the literature. Transl Res Anat. 2021;23:100107. https://doi.org/10.1016/j.tria.2020.100107.
15. Bednarz M, Gromaszek M, Daniluk A, Iwaniuk K, Samczuk M, Białkowska Z, et al. Superior thyroid artery – variations of origin and clinical significance. J Pre Clin Clin Res. 2024;18(2):168-74. https://doi.org/10.26444/jpccr/188620.
16. Zaccheo F, Mariotti F, Guttadauro A, Passaretti A, Campogrande ME, et al. A rare configuration origin of the superior thyroid, lingual and facial arteries in a pentafurcated common carotid artery. Anatomia. 2022;1(2):204-209. https://doi.org/10.3390/anatomia102002016.
17. Kaneko K, Akita M, Murata E, Imai M, Sowa K. Unilateral anomalous left common carotid artery; a case report. Ann Anat. 1996;178(5):477-80. doi: 10.1016/S0940-9602(96)80147-6.
18. Lo A, Oehley M, Bartlett A, Adams D, Blyth P, Al-Ali S. Anatomical variations of the common carotid artery bifurcation. ANZ J Surg. 2006;76(11):970-2. doi: 10.1111/j.1445-2197.2006.03913.x.
19. Ogeng’o JA, Misiani MK, Loyal P, Ongeti KW, Gimongo J, Inyimili MI, et al. Variant termination of the common carotid artery: cases of quadrifurcation and pentafurcation. Anat J Af. 2014;3(3 Suppl):386-392.
20. Gupta P, Bhalla AS, Thulkar S, Kumar A, Mohanti BK, Thakar A, Sharma A. Variations in superior thyroid artery: a selective angiographic study. Indian J Radiol Imaging. 2014;24(1):66-71. doi: 10.4103/0971-3026.130701.
21. Vázquez T, Cobiella R, Maranillo E, Valderrama FJ, McHanwell S, Parkin I, Sañudo JR. Anatomical variations of the superior thyroid and superior laryngeal arteries. Head Neck. 2009;31(8):1078-85. doi: 10.1002/hed.21077.
22. Calotă RN, Rusu MC, Rusu MI, Dumitru CC, Vrapciu AD. Anatomical variables of the superior thyroid artery on computed tomography angiograms. Medicina (Kaunas). 2025;61(5):775. doi: 10.3390/medicina61050775.
23. Poutoglidis A, Savvakis S, Karamitsou P, Forozidou E, Paraskevas G, Lazaridis N, Fyrmpas G, Karamitsou A, Skalias A. Is the origin of the superior thyroid artery consistent? A systematic review of 5488 specimens. Am J Otolaryngol. 2023;44(2):103823. doi: 10.1016/j.amjoto.2023.103823.
24. Herrera-Núñez M, Menchaca-Gutiérrez JL, Pinales-Razo R, Elizondo-Riojas G, Quiroga-Garza A, Fernandez-Rodarte BA, Elizondo-Omaña RE, Guzmán-López S. Origin variations of the superior thyroid, lingual, and facial arteries: a computed tomography angiography study. Surg Radiol Anat. 2020;42(9):1085-1093. doi: 10.1007/s00276-020-02507-6.
25. Tzortzis AS, Antonopoulos I, Pechlivanidou E, Chrysikos D, Pappas N, Troupis T. Anatomical variations of the superior thyroid artery: a systematic review. Morphologie. 2023;107(358):100597. doi: 10.1016/j.morpho.2023.03.002.
26. Tsakotos G, Triantafyllou G, Vlychou M, Vassiou K, Kalamatianos T, Piagkou M. An ectopic thyrolingual trunk arising from the common carotid artery: a rare variant. Surg Radiol Anat. 2024;46(8):1301-1303. doi: 10.1007/s00276-024-03426-6.
27. Kapre M, Mangalgiri AS, Mahore D. Study of thyro-lingual trunk and its clinical relevance. Indian J Otolaryngol Head Neck Surg. 2013;65(2):102-4. doi: 10.1007/s12070-011-0411-7.
28. Jadhav SD, Ambali MP, Patil RJ. Anatomical variation of the origin of the right lingual artery. Int J Anat Var. 2011;4:75-8.