

Introduction
Community-acquired pneumonia (CAP) represents a significant public health concern due to its steadily rising incidence, estimated at 5-12 cases per 1,000 individuals. It remains the leading cause of mortality among infectious diseases and ranks as the sixth among the primary causes of death globally. The incidence of CAP increases markedly with age, reaching 25-40% in individuals over 65 years [1].
Several risk factors are associated with unfavorable outcomes in CAP, with pre-existing cardiovascular disease being the most significant. Elderly patients (over 65 years) frequently present with comorbidities, the most prevalent being chronic obstructive pulmonary disease, ischemic heart disease, chronic congestive heart failure, diabetes mellitus, and cerebrovascular disease [2].
Chronic heart failure (CHF) is a widespread clinical syndrome, particularly among the elderly. Its prevalence in the general population is estimated at 2-3%, with a sharp increase in individuals aged 70-80 years, reaching 10-20%. Among these patients, the four-year mortality rate approaches 50% [3]. The diagnosis of CHF is complex and requires a combination of clinical evaluation and objective evidence of cardiac dysfunction. Diagnostic confirmation is supported by paraclinical investigations such as electrocardiography, chest radiography, and echocardiography, alongside laboratory testing, including complete blood counts, biochemical markers, and natriuretic peptide levels. A favorable clinical response to appropriate therapy further strengthens the diagnosis [4].
Oxidative stress (OS) and reactive oxygen species (ROS) are central to the mechanisms underlying cellular dysfunction and tissue injury. ROS contribute significantly to the inflammatory cascade triggered by bacterial infections [5]. Furthermore, ROS influence intracellular signaling pathways, leading to the activation of transcription factors and the release of pro-inflammatory mediators. Despite the recognized role of oxidative stress in both CAP and CHF, current literature provides limited insight into its dynamics in patients with co-existing CAP and CHF [6, 7].
The interest in knowing the different patterns of inflammation and their related factors has led to a better understanding of the immunopathogenic process that occurs in CAP. The natural course of the infection and its systemic inflammatory pattern in patients with concomitant CHF remain poorly studied [8]. Our first hypothesis is that patients with CAP and CHF have an expressed inflammatory response. And the second hypothesis of our study is that this group of patients have increased levels of oxidative markers. So far, there is a lack of published data about this aspect, which we considered key for interpreting the inflammatory and oxidative stress pattern in patients with CAP and CHF.
Material and methods
This is a prospective, observational, analytic cohort study, conducted in the Department of Internal Medicine, Holy Trinity Municipal Clinical Hospital, Chisinau, Republic of Moldova, during October 2021 – October 2022. The study design included 210 patients hospitalized with CAP, divided into two groups according to the presence of chronic heart failure: Group 1 – 105 patients with CAP and CHF (study group), Group 2 – 105 patients with CAP and without CHF (control group). The study was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy, No.18 from April 12, 2019.
Study inclusion criteria were: patients with and without chronic heart failure with community-acquired pneumonia and mandatory presence of clinical and paraclinical features for pneumonia – acute onset, physical pulmonary consolidation syndrome, pulmonary infiltrate at the chest X-ray; presence of criteria for chronic heart failure (edema, dyspnea, cough, wet rales in the lower lungs, decreased exercise tolerance); previously established chronic heart failure (confirmed by medical records such as outpatient charts or hospital discharge summaries); patient age over 50 years; ability of patients to communicate well with the researcher and the ability to understand and comply with the requirements of the study; signed informed consent for inclusion in the study.
We determined the values of prooxidant markers: ischemic modified albumin (IMA), advanced glycation end-products (AGE), advanced oxidation protein products (AOPP), malonic dialdehyde (MDA), and antioxidant markers: total antioxidant activity (TAA) with CUPRAC and ABTS methods, superoxide dismutase (SOD) and catalase. Inflammatory status was assessed by determining leukocyte count, erythrocyte sedimentation rate (ESR), lactate dehydrogenase (LDH), fibrinogen, C-reactive protein (CRP). Additionally, N-terminal pro-B-type natriuretic peptide (NT-pro-BNP) values were determined in all patients.
Statistical analysis was performed using IBM SPSS Statistics 26.0 and Microsoft Office Excel 2010. All results are presented as M ± m, where M is the sample mean and m is the error of the mean. The following methods were used for statistical data processing: Fisher test (or Fisher-Irwin test, exact χ² test) for non-parametric data and One-Way ANOVA test ("analysis of variance") for parametric data.
Results
The age of patients in the study group ranged from 50 to 92 years, with a mean of 70.6 ± 8.89 years (95% CI [68.8-72.3]; Mn = 70.0; IQRR = 11). In the control group, the mean age was 68.7 ± 7.56 years (95% CI [64.2-68.2]; Mn = 68.0; IQRR = 11) (F = 18.109; p = 0.205). The proportion of women in Group 1 was higher than that of men, at 57 (54.3%; CI 95% [44.8-64.1]) and 48 (45.7%; CI 95% [35.9-55.2]). In Group 2 there were more men than women: 54 (51.4%; CI 95% [42.3-61.0]) and 51 (48.6%; CI 95% [39.0-57.7]), respectively, (χ2 = 0.686; df = 1; p = 0.407) (Fig. 1).
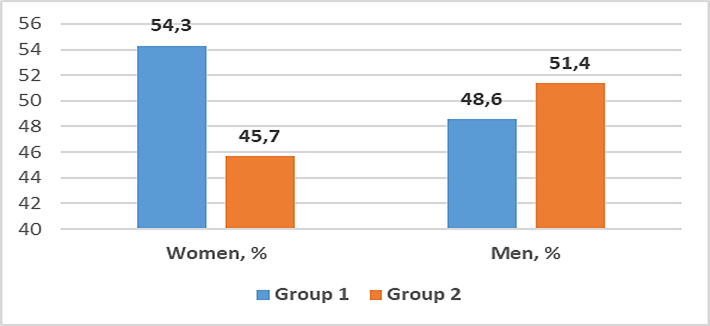 |
Fig. 1. Distribution of subjects with community-acquired pneumonia and chronic heart failure according to gender. Note: The diagram illustrates gender distribution among studied patients. The proportion of women in Group 1 exceeded that of men, while the opposite was true for Group 2. Data are presented in percentages (%). |
Assessing the severity of chronic heart failure according to the New York Heart Association (NYHA) classification in the study group, the following were found: NYHA class II was present in 42 (40.0%; 95% CI [30.5-49.5]) patients, and NYHA class III in 63 (60.0%; 95% CI [50.5-69.5]) patients. According to etiology, CHF had several causes: ischemic – 16 patients (15.2%; 95% CI [8.8-22.2]), valvular – 1 patient (1.0%; 95% CI [0.0-3.2]), and mixed – 88 patients (83.8%; 95% CI [76.6-90.7]).
Patients with community-acquired pneumonia and chronic heart failure had a longer hospital stay, compared to those without CHF: 11.96 ± 0.36 versus 10.82 ± 0.28 days, which was statistically significant (F = 6.020; p = 0.012).
On the objective examination of the respiratory system in Group 1, we determined that 21 (20.0%; 95% CI [12.3-28.4]) patients presented increased vocal fremitus, increased vesicular murmur – 37 (35.2%; 95% CI [26.0-44.4]) patients, dullness – 13 (12.4%; 95% CI [6.5-18.8]) patients, decreased local vesicular murmur – 74 (70.5%; 95% CI [60.6-78.6]) patients. Unilateral crepitant rales were observed in 27 (25.7%; 95% CI [17.9-35.2]) patients, bilateral – 41 (39.0%; 95% CI [30.6-48.6]) patients, sibilant rales were present in 6 (5.7%; 95% CI [1.8-10.5]) patients. No statistical significance was found between the groups.
Arterial hypertension was the most common comorbidity in the study group – 103 (98.0%) patients, compared to 84 (80.1%) patients in the control group. Diabetes mellitus was found in 41 (39.0%; 95% CI [29.9-48.4]) patients in the study group, occurring twice as frequently as in the control group, where it was present in only 25 (23.8%; 95% CI [15.8-32.4]) patients (p = 0.017). Cerebrovascular disease was present in 47 (44.8%; 95% CI [35.5-54.3]) patients in the study group and in 25 (23.8%; 95% CI [16.0-32.3]) patients in the control group (p = 0.001). Simple chronic bronchitis occurred less frequently in patients in Group 1 compared to Group 2: 29 (27.6%; 95% CI [19.6-35.6]) and 39 (37.1%; 95% CI [28.2-46.9]), respectively (p = 0.140). Chronic kidney disease occurred more frequently in Group 1 compared to Group 2: 21 (20.0%; 95% CI [12.6-27.4]) patients and 6 (5.7%; 95% CI [1.9-10.8]) patients, respectively (p = 0.002). Atrial fibrillation was present only in Group 1 – 54 (51.4%; 95% CI [42.2-61.0]) patients, p < 0.0001.
An important aspect explored in the study, was the radiological picture in patients with CAP and CHF, represented by alveolar infiltrate, identified in 38 (36.2%; 95% CI [27.3-45.1]) patients in the study group (p = 0.886), while interstitial infiltrate was found in 67 (63.8%; 95% CI [54.9-72.7]) patients (p = 0.885). Bilateral infiltrate extent was more frequently observed in patients with CAP and CHF – 63 (60.0%; 95% CI [50.5-69.1]) patients – followed by polysegmental involvement in 27 (25.7%; 95% CI [17.7-34.3]) patients, segmental involvement (1-2 segments) in 10 (9.5%; 95% CI [4.3-15.5]) patients, and lobar involvement in 5 (4.8%; 95% CI [1.0-9.3]) patients, also without significant differences between groups. Pleural effusion was significantly higher in patients in the study group compared to those in the control group: 41 (39.0%; 95% CI [30.6-49.5]) patients and 14 (13.3%; 95% CI [7.3-20.0]) patients, respectively (χ² = 17.958; df = 1; p < 0.0001).
Significant differences between groups were observed in relation to the mean value of NT-pro-BNP. Thus, in Group 1, NT-pro-BNP had a mean value of 1371.88 ± 498.91 pg/mL, compared to Group 2: 58.19 ± 48.22 pg/mL, (F = 721.542; p < 0.0001), with a threshold value of NT-pro-BNP in patients with CHF and severe course of CAP of 1665.73 pg/mL.
There were no statistical differences between groups in terms of leukocyte counts, with a mean of 10.36 ± 7.13 × 109/L and 10.52 ± 5.58 × 109/L in both groups, respectively (F = 0.033; p = 0.856). Increased inflammatory status was determined by higher serum LDH values in the CHF group, compared to the control group: 232.65 ± 109.80 units/L and 192.40 ± 44.98 units/L, respectively, (F = 12.076; p = 0.001) (Fig. 2.).
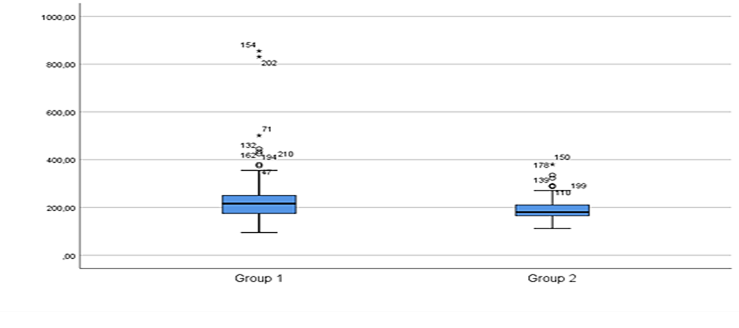 |
Fig. 2. Lactate dehydrogenase levels in patients with community-acquired pneumonia and chronic heart failure, u/L. Note: The boxplot illustrates lactate dehydrogenase levels in patients with CAP and CHF. Group 1 shows a higher median LDH level and greater variability. In contrast, Group 2 has a slightly lower median and a narrower interquartile range. The following statistical data were calculated: median, interquartile range, minimum and maximum values. |
The mean ESR value was significantly higher in Group 1 compared to Group 2: 29.89 ± 15.98 mm/h and 21.17 ± 19.47 mm/h, (F = 12.561; p < 0.0001), and the median values were as follows: Mn = 17.0; IQR = 20.0 compared to Mn = 26.0; IQR = 29.0, respectively. The mean fibrinogen values were also higher in Group 1 (5.24 ± 1.60 g/L), compared to Group 2 (4.51 ± 1.78 g/L), (F = 9.692; p = 0.002).
Analyzing changes in oxidative status, we determined a more pronounced pro-oxidative markers, manifested by higher values of ischemic modified albumin in patients in Group 1 compared to Group 2: 236.60 ± 57.23 µM/L and 229.77 ± 64.35 µM/L, respectively, (F = 0.660; p = 0.045). The threshold value of IMA in patients with CHF and severe course of CAP was 218.98 µM/L.
AGE-pentosidine-like, AGE-vesperlysine-like values, advanced oxidation protein products, malonic dialdehyde values showed no statistically significant differences between the groups (Table 1).
Table 1. Comparison of oxidative stress markers in patients with community-acquired pneumonia and chronic heart failure. | ||||||
Oxidative stress parameters | Group 1 (n = 105) | Group 2 (n = 105) | F | P | ||
Mean | SD ± | Mean | SD ± | |||
IMA, µM/L | 236.6077 | 57.23919 | 229.7775 | 64.35578 | 0.660 | 0.045 |
AGE- pentosidin-like, µM/L | 598.7908 | 251.68051 | 544.5575 | 197.20439 | 3.021 | 0.084 |
AGE- verperlisin-like, µM/L | 449.1497 | 169.38287 | 455.2475 | 160.66932 | 0.072 | 0.789 |
AOPP, µM/L | 95.2128 | 63.05108 | 105.9567 | 55.21101 | 1.726 | 0.190 |
MDA, µM/L | 17.4629 | 6.94660 | 16.0739 | 4.72922 | 2.869 | 0.092 |
Catalase, µM/L | 21.8819 | 10.01078 | 23.1646 | 11.54527 | 0.740 | 0.391 |
TAA with CUPRAC, µM/L | 6.7012 | 4.62461 | 4.9987 | 2.29101 | 7.647 | 0.006 |
TAA with ABTS, µM/L | 132.2233 | 21.48573 | 128.2355 | 22.21592 | 1.748 | 0.188 |
SOD, units/g | 62.7206 | 13.37431 | 62.3362 | 16.47029 | 0.034 | 0.853 |
Note: IMA - ischemic modified albumin; AGE - advanced glycation end-products; AOPP - advanced oxidation protein products; TAA - total antioxidant activity; SOD - superoxide dismutase; MDA - malonic dialdehyde. The table presents the oxidative markers changes in patients with CAP and CHF, manifested through increased IMA levels and counterbalanced by antioxidant system – increased TAA with CUPRAC method. For data analysis it was used One-Way ANOVA statistical test. | ||||||
Further, we analyzed the values of antioxidant markers. The counterbalancing of antioxidant status was determined through a higher total antioxidant activity with CUPRAC method in patients from Group 1 (6.70 ± 4.62 µM/L) compared to Group 2 (4.99 ± 2.29 µM/L), (F = 7.647; p = 0.006) (Fig. 3.).
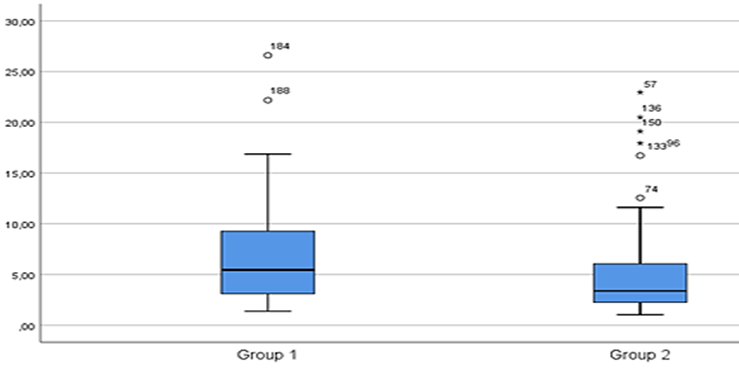 |
Fig. 3. Total antioxidant activity with CUPRAC method in patients with community-acquired pneumonia and chronic heart failure, compared to the control group. Note: The boxplot illustrates total antioxidant activity with CUPRAC method levels in patients with CAP and CHF. Group 1 shows a higher median antioxidant activity and greater variability compared to Group 2. The following statistical data were calculated: median, interquartile range, minimum and maximum values. |
Total antioxidant activity using the ABTS method was also higher in patients with CHF (132.22 ± 21.48 µM/L) compared to those without CHF (128.23 ± 22.21 µM/L), (F = 1.748; p = 0.188). Superoxide dismutase values were not significantly different between Group 1 and Group 2: 62.72 ± 13.37 units/g and 62.33 ± 16.47 units/g, respectively. At the same time, catalase levels were lower in patients in Group 1 (21.88 ± 10.01 µM/L) compared to Group 2 (23.16 ± 11.54 µM/L), (F = 0.740; p = 0.391)
In patients with CAP and concomitant CHF, total antioxidant activity determined by the CUPRAC method had a significant positive correlation with atrial fibrillation (rs = 0.343; p = 0.038), arterial hypertension (rs = 0.329; p = 0.001), worsening of pre-existing dyspnea (rs = 0.308; p = 0.002), and the presence of pericardial effusion (rs = 0.357; p = 0.023).
At the same time, ischemic modified albumin showed a significant positive correlation with radiological extension of the pulmonary infiltrate (rs = 0.435; p = 0.010) and with fibrinogen levels (rs = 0.387; p = 0.050). Advanced oxidation protein products had a positive correlation with total hospital length of stay (rs = 0.341; p = 0.041). AGE-pentosidine-like compounds showed a significant positive correlation with the presence of pleural effusion on chest X-rays (rs = 0.334; p = 0.001). Lactate dehydrogenase levels had a positive correlation with radiological extent of the pulmonary infiltrate (rs = 0.394; p = 0.025).
Discussions
In our analysis of comorbidities among patients with community-acquired pneumonia and chronic heart failure, hypertension emerged as the most prevalent coexisting condition, identified in 98.0% of cases. This data are similar to the results of a systematic review and meta-analysis, that investigated the impact of comorbidities and risk factors on community-acquired pneumonia in the Indian population. Analyzing 23 observational studies published between 1990 and 2021, the study found that the most common comorbidities among CAP patients were chronic obstructive pulmonary disease (24.2%), hypertension (23.7%), and diabetes mellitus (16%) [9, 10].
In our study, radiologic findings in patients with community-acquired pneumonia and chronic heart failure revealed interstitial-type infiltrates in most of the patients. The most frequent distribution pattern was bilateral involvement, followed by polysegmental extension, segmental involvement and lobar involvement. Bobilev et al. conducted a study to evaluate the clinical features and progression of community-acquired pneumonia in patients with chronic heart failure, reporting alveolar infiltrates in 60% of cases and interstitial infiltrates in 32% [11]. Pleural effusion was determined in 41 patients (39.0%) with community-acquired pneumonia and chronic heart failure. In contrast, a prospective cohort study by Bartoli A. et al., which investigated pleural effusion in hospitalized patients with decompensated chronic heart failure, reported a higher prevalence—67.5%, with bilateral effusion in 53.6% of cases and unilateral effusion in 15.6% [12, 13].
The results of our study demonstrate that NT-proBNP levels were higher in patients with CAP and CHF and correlated positively with radiological extent of the pulmonary infiltrate and with pneumonia severity. This data is supported by Li J et al., who aimed to evaluate, whether plasma B-type natriuretic peptide levels can accurately predict the severity of CAP, and showed that BNP levels strongly correlated with CAP severity and mortality risk. A BNP threshold of ≥125 pg/mL may flag high-risk patients, while ≥299 pg/mL indicates elevated risk of death [14]. Also, NT-proBNP had a strong predictive value for 30-day mortality in hospitalized CAP patients, with an area under the curve (AUC) of 0.735 [95% CI (0.642–0.828)], p < 0.001. The optimal NT-proBNP cut-off for predicting both ICU admission and 30-day mortality was 1,434.5 pg/mL [15].
Laboratory analysis in our study showed that mean fibrinogen levels were higher in patients with concomitant chronic heart failure, suggesting an increased inflammatory response in this population. These results can be explained by an acute-phase response and systemic inflammation in patients with CAP associated with the low-grade systemic inflammation, determined in CHF. Our data is supported by a study that aimed to evaluate the prognostic value of fibrinogen levels in patients with acute exacerbation of chronic heart failure. A total of 554 patients were analyzed and stratified into two groups based on fibrinogen levels: low (≤284 mg/dL) and high (≥284 mg/dL), with the cut-off determined by ROC curve analysis. The area under the curve for predicting 90-day mortality was 0.65 (95% CI; 0.59–0.70). High fibrinogen levels were significantly associated with increased 90-day mortality, with an unadjusted hazard ratio of 3.33 (95% CI; 2.15–5.15). The study concluded that elevated fibrinogen is an independent predictor of 90-day mortality in chronic heart failure population [16].
Our study also demonstrated significantly elevated lactate dehydrogenase levels in patients with community-acquired pneumonia and chronic heart failure compared to the control group. A related study examined the predictive value of LDH, C-reactive protein and neutrophil counts in assessing the severity of community-acquired pneumonia. Reported LDH levels ranged from 266 to 1,424 U/L, with a mean of 598.1 ± 286.79 U/L, while CRP values ranged from 22.75 to 202.25 mg/L, averaging 53.5 ± 23.14 mg/L. The study found a significant positive correlation between neutrophil count, LDH, CRP, and the CURB-65 severity score [17].
Subsequently, we analyzed oxidative damage markers (ischemic-modified albumin, advanced glycation end products, advanced oxidation protein products, malonic dialdehyde) in patients with CAP and CHF. Ischemic modified albumin, which is evaluated as a cardiac ischemia marker, was more pronounced in patients with CAP and CHF compared to the control group and showed a significant positive correlation with radiological extension of the pulmonary infiltrate. Our results are supported by a study, that aimed to evaluate the diagnostic utility of IMA levels in patients with CAP presenting to the Emergency Department and included 162 adult participants: 81 patients diagnosed with CAP and 81 healthy controls. The results showed significantly elevated IMA levels in CAP patients (0.532 ± 0.117 IU/mL) compared to controls (0.345 ± 0.082 IU/mL), p < 0.05. An IMA cutoff value of 0.442 IU/mL yielded a sensitivity of 75.3% and a specificity of 91.3% for CAP diagnosis. A moderate positive correlation was observed between IMA and CRP levels (r = 0.506, p < 0.05). These data suggest that IMA may serve as a novel and practical biomarker to aid in the early diagnosis of CAP [18, 19].
In our study, the antioxidant defense system in patients with community-acquired pneumonia and chronic heart failure was evaluated through measurements of total antioxidant activity using the CUPRAC and ABTS methods, both of which showed elevated levels. However, catalase activity was found to be reduced in the CHF group. The increased antioxidant activity observed may reflect a compensatory response to oxidative stress, driven by an imbalance between the heightened production of reactive oxygen species and the limited capacity for their elimination or neutralization – potentially linked to hypoxia, as suggested by elevated LDH levels [20, 21].
In the present study, it is necessary to mention the difficulty of collecting biological material in some cases, , due to the overlap of study collection with the COVID-19 pandemic. Thus, during that period, sputum collection for microscopic and bacteriological examination was restricted. There were also limitations regarding the measurament of serum procalcitonin, as well as performing chest computed tomography.
Conclusions
Community-acquired pneumonia in patients with chronic heart failure is associated with an enhanced inflammatory response, as demonstrated by elevated lactate dehydrogenase, erythrocyte sedimentation rate and fibrinogen levels. Furthermore, increased oxidative stress is indicated by significantly elevated levels of ischemic modified albumin, which positively correlated with the radiological extent of pulmonary infiltrates. Ischemic modified albumin may serve as a novel and practical biomarker to support the early diagnosis of community-acquired pneumonia in patients with chronic heart failure.
Competing interests
None declared.
Authors’ contributions
VC conceived the study and participated in study design. TD helped drafting the manuscript and participated in data analysis. DF had a substantial contribution to acquisition of data. SM and LG contributed to final approval of the version to be published. All the authors reviewed the work critically and approved the final version of the manuscript.
Ethics approval
The research project was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (Minutes no. 18 from 12.04.2019).
Patient consent
Obtained.
Acknowledgements and funding
No external funding.
Provenance and peer review
Not commissioned, externally peer reviewed.
Authors’ ORCID IDs
Virginia Cascaval – https://orcid.org/0009-0008-5899-100X
Tatiana Dumitras – https://orcid.org/0000-0001-5538-189X
Diana Fetco-Mereuta – https://orcid.org/0000-0002-7469-045X
Sergiu Matcovschi – https://orcid.org/0000-0003-1623-930X
Livi Grib – https://orcid.org/0000-0001-6913-0864
References
Divino V, Schranz J, Early M, et al. The annual economic burden among patients hospitalized for community-acquired pneumonia (CAP): a retrospective US cohort study. Curr Med Res Opin. 2020;36(1):151-160. doi: 10.1080/03007995.2019.1675149.
Marin-Corral J, Pascual-Guardia S, Amati F, et al. Aspiration risk factors, microbiology, and empiric antibiotics for patients hospitalized with community-acquired pneumonia. Chest. 2021;159(1):58-72. https://doi.org/10.1016/j.chest.2020.06.079.
Shen L, Jhund P. S, Anand I. S, et al. Incidence and outcomes of pneumonia in patients with heart failure. Journal of the american college of cardiology. 2021;77(16):1961-1973. https://doi.org/10.1016/j.jacc.2021.03.001.
Mancini D, Gibson G. Impact of pneumonia in heart failure patients. J Am Coll Cardiol. 2021;77(16):1974-1976. https://doi.org/10.1016/j.jacc.2021.03.010.
Carr AC, Spencer E, Dixon L, et al. Patients with community acquired pneumonia exhibit depleted vitamin C status and elevated oxidative stress. Nutrients. 2020;12(5):1318. https://doi.org/10.3390/nu12051318.
Zhang Q, Ju Y, Ma Y, Wang T. N-acetylcysteine improves oxidative stress and inflammatory response in patients with community acquired pneumonia: a randomized controlled trial. Medicine (Baltimore). 2018;97(45):e13087. doi: 10.1097/MD.0000000000013087.
Cascaval V, Matcovschi S, Grib L, et al. Oxidative stress in patients with community-acquired pneumonia and pre-existing heart failure. Arch Balk Med Union. 2024;59(4):336-342. https://doi.org/10.31688/ABMU.2024.59.4.02.
Méndez R, Menéndez R, Cillóniz C, et al. Initial inflammatory profile in community-acquired pneumonia depends on time since onset of symptoms. Am J Respir Crit Care Med. 2018;198(3):370-378. https://doi.org/10.1164/rccm.201709-1908OC.
Ghia CJ, Rambhad GS. Systematic review and meta-analysis of comorbidities and associated risk factors in Indian patients of community-acquired pneumonia. SAGE Open Med. 2022;10. doi: 10.1177/20503121221095485.
Cha YS, Lee KH, Lee JW, et al. The usefulness of the delta neutrophil index for predicting superimposed pneumonia in patients with acute decompensated heart failure in the emergency department. PLoS One. 2016;11(9):e0163461. doi: 10.1371/journal.pone.0163461.
Bobylev A, Rachina S, Avdeev S, et al. Etiologiia vnebol’nichnoi pnevmonii u lits s khronicheskoi serdechnoi nedostatochnost’iu [Etiology of community-acquired pneumonia in patients with chronic heart failure]. Pulmonologiya. 2019;29(3):293-301. https://doi.org/10.18093/0869-0189-2019-29-3-293-301. Russian.
Bartoli A, Donadoni M, Ceriani E, et al. Phenotyping pleural effusion in patients hospitalized in Internal Medicine wards with decompensated heart failure. Eur J Intern Med. 2024;120:131-133. doi: 10.1016/j.ejim.2023.11.008.
Marinkovic SP, Topuzovska IK, Stevanovic M, et al. Features of parapneumonic effusions. Pril Makedon Akad Nauk Umet Odd Med Nauki. 2018;39(1):131-141. doi: 10.2478/prilozi-2018-0033.
Li J, Ye H, Zhao L. B-type natriuretic peptide in predicting the severity of community-acquired pneumonia. World J Emerg Med. 2015;6(2):131-6. doi: 10.5847/wjem.j.1920-8642.2015.02.008.
Akpınar EE, Hoşgün D, Akpınar S, et al. Do N-terminal pro-brain natriuretic peptide levels determine the prognosis of community acquired pneumonia? J Bras Pneumol. 2019;45(4):e20180417. https://doi.org/10.1590/1806-3713/e20180417.
Meng Z, Zhao Y, He Y. Fibrinogen Level Predicts Outcomes in Critically Ill Patients with Acute Exacerbation of Chronic Heart Failure. Dis Markers. 2021; 2021:6639393. doi: 10.1155/2021/6639393.
Hendy RM, Elawady MA, EL Kareem HMA. Role of lactate dehydrogenase and other biomarkers in predicting prognosis of community-acquired pneumonia. Egypt J Bronchol. 2019;13:539-544. https://doi.org/10.4103/ejb.ejb_22_19.
Bolatkale M, Duger M, Ülfer G, et al. A novel biochemical marker for community-acquired pneumonia: Ischemia-modified albumin. The American journal of emergency medicine. 2017;35(8):1121-1125. https://doi.org/10.1016/j.ajem.2017.03.018.
Cascaval V, Dumitras T, Fetco-Mereuta D, et al. Clinical-radiological features and oxidative stress in patients with community-acquired pneumonia and heart failure. Pneumologia. 2024;73:1-7. https://doi.org/10.2478/pneum-2025-0001.
Fetco-Mereuta D, Dumitras T, Grib L, et al. Clinical and paraclinical approach to community-acquired pneumonia in obese individuals. Mold J Health Sci. 2024;11(2):3-7. https://doi.org/10.52645/MJHS.2024.2.01.
Reshetar DV. Indices of the oxidant and antioxidant system and endogenous intoxication in the convalescents after community-acquired pneumonia. Galician Med J. 2015;22(1):115-118. https://ifnmujournal.com/gmj/article/view/276.