
Introduction
Healthcare-associated bloodstream infections (HA-BSIs) are among the most severe complications of modern medical care, particularly in pediatric patients. They significantly contribute to increased morbidity, mortality, prolonged hospitalization, and higher treatment costs [1-3]. Bloodstream infections, including central line-associated bloodstream infections (CLABSIs), represent the most frequent type of healthcare-associated infections (HAIs) in neonates admitted to neonatal intensive care units (NICUs) [4, 5], with considerable variation depending on region and the development level of the healthcare system [6]. According to ECDC data, 6.4% of patients admitted to intensive care units (ICUs) develop BSIs if hospitalization exceeds two days [7].
A review of the literature estimated between 575,000 and 677,000 episodes of BSIs annually in North America (536,000–628,000 in the U.S. and 40,000–49,000 in Canada), associated with 79,000–94,000 deaths (72,000–85,000 in the U.S. and 7,000–9,000 in Canada), and more than 1.2 million BSI episodes and 157,000 deaths per year occurring in Europe. BSIs have a major global impact on morbidity and mortality and are ranked among the top seven causes of death worldwide [8]. In the United States, the annual mortality rate associated with BSIs is estimated at 23.5–27.5 deaths per 100,000 population – surpassing the number of deaths caused by any other infectious disease, including influenza and pneumonia combined (16.2 deaths per 100,000) [8]. In Europe, BSIs are the second leading cause of disability and premature death and are also associated with the highest number of preventable deaths among HAIs [9]. The costs associated with BSIs vary widely, with estimates ranging from $960 million to $18.2 billion annually [10].
These infections are often caused by the use of central and peripheral venous catheters, which allow direct access for pathogenic microorganisms into the bloodstream [11, 12]. According to data from the literature, approximately 36.7% of BSI cases are attributed to vascular catheter use, of which 28.4% are associated with central venous catheters and 8.3% with peripheral ones. Additionally, 32.4% of cases occur secondary to other preexisting infections [13]. The incidence of catheter-associated infections varies considerably, ranging from 1.6 to 44.6 CLABSIs per 1,000 catheter-days in adult and pediatric ICUs, and from 2.6 to 60.0 CLABSIs per 1,000 catheter-days in NICUs [14].
This study aims to provide a systematic review of the literature regarding the incidence, causative pathogens, risk factors, and effective strategies to reduce healthcare-associated bloodstream infections in children, in order to improve prevention and management practices in pediatric healthcare settings.
Materials and methods
To conduct this literature review study, an advanced search was performed in the electronic databases PubMed, SCOPUS, and Web of Science using the following keywords: “bloodstream infections,” “antimicrobial resistance,” “pediatric patients,” “healthcare-associated infections,” “mortality,” “length of hospital stay,” and “costs”, in combination with the Boolean operators “AND,” “OR,” and “NOT.” The search yielded a total of 957 publications – 549 from PubMed, 284 from SCOPUS, and 124 from Web of Science. Of these, 23.72% (n = 227) were duplicates.
The remaining articles were screened following the PRISMA guidelines [15]. In the initial screening phase, 730 publications were reviewed, of which 75.2% (n = 549) did not meet the study objective. A total of 181 scientific papers were assessed for eligibility based on the following inclusion criteria:
Articles published between 2010 and 2024.
Language of publication: English and/or Romanian.
Open-access publications.
Types of articles: literature reviews, research articles, and meta-analyses.
The following were excluded from the review: articles published in Russian, French, Polish, Chinese, Turkish, Spanish, and Italian; publications dated between 1980 and 2009; editorial letters and article corrections; and restricted-access papers (Figure 1).
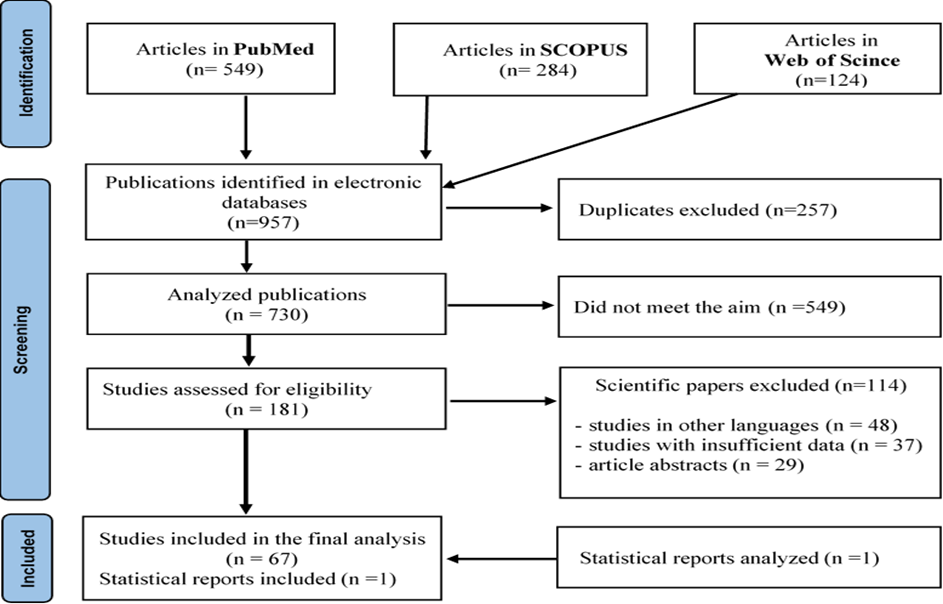 |
Fig. 1 Publication selection criteria according to the PRISMA 2020 guidelines |
A total of 67 publications were selected for the final study. The analysis of the national epidemiological situation was carried out based on data collected from Statistical Form No. 2, “Report on selected infectious and parasitic diseases registered in the Republic of Moldova” for the year 2023, as provided by the National Agency for Public Health.
Results
The literature review highlighted the main epidemiological characteristics of the epidemic process caused by healthcare-associated bloodstream infections in pediatric patients. Epidemiological data were extracted from 67 scientific articles that met the inclusion criteria established for this study. In the Republic of Moldova, HA-BSIs and, more broadly, healthcare-associated infections in children remain an underexplored topic. Therefore, we aimed to identify the key epidemiological features, risk factors, and strategies for the prevention and control of HA-BSIs in the pediatric population, based on internationally published scientific evidence.
In 2012, the International Nosocomial Infection Control Consortium (INICC) reported device-associated infection rates in 16 PICUs in low- and middle-income countries (LMICs), revealing significantly higher values compared to high-income countries. According to INICC data, the incidence of ventilator-associated pneumonia (VAP) was 6 infections per 1,000 device-days, CLABSIs had a rate of 8.1 infections per 1,000 device-days, and catheter-associated urinary tract infections (CAUTIs) were reported at 4.1 infections per 1,000 device-days [12]. In contrast, PICUs in the United States reported significantly lower rates: 0.7 for VAP, 1.0 for CLABSI, and 3.5 for CAUTI. These marked differences reflect the challenges that LMIC healthcare systems face in terms of infection prevention and control. Furthermore, the actual burden of these infections in LMICs is likely underestimated, considering that 75% of the PICUs included in the INICC report were located in private hospitals, where practices and resources may differ significantly from those in the public sector [13].
Another study conducted in a developing country found that 56.5% of HAIs occurred in children under 1 year of age, and the incidence density of BSIs in children was 18.1 per 1,000 central venous catheter (CVC) days. Of all identified HAIs, 60.49% were BSIs, and most of them (38 out of 49) were associated with the use of venous catheters. Moreover, bloodstream infections were significantly more common in children with CVCs than in those without (20% vs. 4.7%, p < 0.05) [5].
According to a study conducted in Brazil as part of the SCOPE project, out of a total of 342 bloodstream infection episodes, 50.2% occurred in children under one year of age. Nearly half of the patients (45.3%) were admitted to pediatric or neonatal intensive care units, while 21.0% were treated in general pediatric units. Additionally, 66.4% of patients had central venous catheters, 23.1% had peripheral venous catheters, and 2.6% had arterial catheters, highlighting the high prevalence of device-associated infections [16].
Similar results were reported in a study by the European Centre for Disease Prevention and Control (ECDC), which identified 770 cases of HAIs, of which 45% were bloodstream infections. Although most BSIs were reported in infants under 12 months of age, the percentages remained significant across other age groups as well [17].
In another study analyzing children admitted to PICUs, bloodstream infections accounted for 45.4% of all healthcare-associated infections (HAIs), followed by respiratory tract infections (RTIs) at 27.8% and urinary tract infections (UTIs) at 15.8%. Among the 244 BSI cases analyzed, 79.9% were associated with central venous catheter (CVC) use, most of which were diagnosed in patients who had the catheter in place for more than 48 hours [18]. High BSI rates were also reported in a study conducted in Morocco, where these infections represented 44% of HAI cases, followed by nosocomial pneumonia (30%) and surgical site infections and UTIs (each at 7%) [19].
An important aspect regarding the incidence of BSIs is the significant disparity between high-income countries (HICs) and low- and middle-income countries (LMICs). A study conducted in PICUs in LMICs highlighted a significantly higher incidence of HAIs, with CLABSI, VAP, and CAUTI rates all markedly higher compared to HICs: 12.2 vs. 7.0 per 1,000 central line-days; 9.0 vs. 5.4 per 1,000 ventilator-days; and 5.9 vs. 3.7 per 1,000 urinary catheter-days, respectively [20].
Research conducted by Saeghi et al. identified 404 episodes of bacteremia in 272 pediatric patients, of which 82.4% were healthcare-associated, with an incidence rate of 11.1 per 1,000 hospitalizations. Community-onset bacteremia accounted for 17.6% of cases. Almost two-thirds of the patients (85.6%) were under 5 years of age, with 34.4% being infants aged 1 month to 1 year. Underlying comorbidities were identified in 90.6% of patients, the most common being prematurity (26.2%), hematologic malignancies (22.3%), intestinal pathologies (17.6%), and metabolic/genetic syndromes (11.6%). A central venous catheter was present in 45.0% of the BSI cases, and in 7.7% of cases, the source of infection was unidentified [21].
BSIs also predominated in a study conducted at Besat Hospital in western Iran, being the most common infection form in both investigated age groups: 37.38% in children aged 0–4 years and 34.75% in those aged 5–14 years. Escherichia coli was more frequently isolated in girls (25.84% in the 0–4 age group and 24.53% in the 5–14 age group), while Staphylococcus aureus was more common in boys (33.6% in the 0–4 age group and 29.55% in the 5–14 age group) [22].
Despite the significant variation in BSI pathogens among children across different countries, age groups, and clinical settings [23], Gram-positive microorganisms continue to play a dominant role in the onset of healthcare-associated BSIs. One recent study reported that Gram-positive bacteria were responsible for 57.0% of infections, Gram-negative organisms for 40.2%, and Candida species for 2.8%. The most frequently isolated microorganisms were Staphylococcus aureus (26.0%), Escherichia coli (13.0%), coagulase-negative staphylococci (8.3%), and Enterococcus spp. Among S. aureus strains, 26.0% were oxacillin-resistant; however, susceptibility to ceftaroline was nearly universal at 99.8%. Among Gram-negative bacteria, Enterobacteriaceae and Pseudomonas aeruginosa together accounted for over 85% of isolates, all of which were susceptible to ceftazidime-avibactam [24].
Consistent with the above, another study reported that Gram-positive organisms accounted for 56% of all identified isolates, while Gram-negative organisms accounted for 44%. The most common Gram-positive bacteria were Staphylococcus aureus (78%), followed by coagulase-negative staphylococci (CoNS) (12%), Enterococcus faecalis (6%), and Streptococcus pneumoniae (4%). In the European HAI surveillance network, the study by Garcia and data collected from PICUs in France also confirmed the predominance of coagulase-negative staphylococci as the primary etiological agents of bacteremia [25, 26].
Even higher rates of Gram-positive microorganisms were observed in a U.S.-based study, where they accounted for 70.6% of pathogens isolated in healthcare-associated BSIs in children, compared to 29.4% for Gram-negative bacteria. The most frequently identified pathogen was coagulase-negative Staphylococcus (CoNS), isolated in 47.1% of cases, followed by Escherichia coli (8.3%), Staphylococcus aureus (7.0%), Streptococcus pneumoniae (5.9%), Klebsiella spp. (5.6%), and Enterococcus spp. (4.4%). A study analyzing isolation trends between 2015 and 2018 reported a significant decrease in the frequency of CoNS and Serratia marcescens (p < 0.05), alongside a significant increase in the prevalence of E. coli, S. aureus, S. pneumoniae, Enterococcus faecalis, and Enterococcus faecium (p < 0.05) [24].
Nevertheless, it is important to note that over the past decade, there has been a significant increase in the number of Gram-negative microorganisms isolated from children with healthcare-associated infections, a trend increasingly reported in international studies [20, 22, 27-30]. One study confirmed the predominance of Gram-negative bacteria in the etiology of HA-BSIs, highlighting a pattern increasingly emphasized in the literature: 60% of infections were caused by Gram-negative pathogens, compared to 33% by Gram-positive bacteria and 7% by fungal pathogens. Klebsiella pneumoniae (17%), Staphylococcus aureus (14%), and Escherichia coli (9.11%) were the most frequently detected pathogens. The crude mortality rate among children with BSIs was 20% (176/864); multivariate analysis identified HIV infection, fungal and Gram-negative sepsis, and the presence of HAIs as significant predictors of mortality [31].
Evidence of the growing dominance of Gram-negative bacteria in the etiological landscape of pediatric HA-BSIs was also reported in a study where, out of 573 isolated strains, 55% were Gram-negative bacteria, 32% Gram-positive bacteria, and 13% fungi. The most frequently isolated species included Enterobacteriaceae (30.9%), Pseudomonas aeruginosa (19.2%), and Staphylococcus aureus (11.0%) [18]. Similar findings on the spectrum of microorganisms isolated from children with HA-BSIs were reported in the United Kingdom [32], Italy [33], Brazil [16], and the United States, particularly among neonates with very low birth weight (<1500 g) [34].
Despite this global trend, some studies from LMICs found that fungi were the predominant etiological agents of pediatric BSIs. For instance, Candida spp. was the most commonly isolated pathogen (41%) among children with BSIs, followed by coagulase-negative Staphylococcus (17%) [5]. In line with these findings, fungemia was the most common in studies from Turkey [27] and Vietnam [28].
Alarmingly, infections caused by multidrug-resistant (MDR) Gram-negative bacteria have expanded significantly in recent years, becoming a major global public health concern [24, 29]. This trend is further compounded by the high rate of antimicrobial resistance (AMR), which was significantly higher in hospital-acquired infections (70%) compared to community-acquired infections (25%; p < 0.0001). Factors associated with AMR included nosocomial infection, age under one year, HIV infection, and sepsis caused by Gram-negative bacteria [31].
The link between Gram-negative bacilli-caused BSIs and AMR was underscored by a recent U.S. study analyzing 721 E. coli isolates (including 393 associated with BSIs), which reported high rates of non-susceptibility to commonly used empirical antibiotics such as: ampicillin (66.8%) and gentamicin (16.8%), and the presence of extended-spectrum beta-lactamases (ESBLs) in 20% of isolates [30]. In another study conducted in Italy and Brazil, 44% of isolates were MDR; among 175 Enterobacteriaceae isolates, 45% were ESBL-positive. Carbapenem resistance was observed in 2% of Enterobacteriaceae, 42% of P. aeruginosa, and 60% of Acinetobacter baumannii. Among Gram-positive bacteria, 56% of S. aureus strains were methicillin-resistant; however, no vancomycin-resistant Enterococcus spp. were detected. Additionally, of 76 coagulase-negative Staphylococcus (CoNS) isolates, 47 (62%) were classified as multidrug-resistant [18].
According to another study conducted in LMICs, Klebsiella spp. was the most common pathogen isolated from neonates with MDR neonatal sepsis [35]. In contrast, Escherichia coli and methicillin-sensitive Staphylococcus aureus were the most frequently isolated pathogens in children with BSIs in a multicenter US. study [36].
Antimicrobial susceptibility data were also reported in a study from a pediatric hospital in Srinagar. Gram-positive bacteria remained fully susceptible to vancomycin, linezolid, daptomycin, teicoplanin, and tigecycline, with no resistance observed. However, a high rate of methicillin resistance was noted, affecting 72% of S. aureus isolates and 50% of CoNS species. Among Gram-negative bacteria, colistin was the only antibiotic uniformly effective across all isolates. In contrast, high levels of resistance were observed for ampicillin, ceftriaxone, ciprofloxacin, and piperacillin-tazobactam, highlighting the growing challenges in treating infections caused by these organisms [37].
The analysis of pathogen distribution by age revealed marked differences across pediatric age groups. Bloodstream infections caused by Gram-positive bacteria predominated in neonates, accounting for 69.0% of all isolates. The most common pathogens in this group were coagulase-negative Staphylococcus (48.0%), Escherichia coli (11.2%), and Klebsiella pneumoniae (8.3%). CoNS was present in all age groups but showed a decreasing frequency with increasing age, while Staphylococcus aureus showed an upward trend. Streptococcus pneumoniae and Viridans group streptococci were more frequently isolated in children aged 3–5 years (14.3% and 3.7%, respectively), whereas beta-hemolytic streptococci were more prevalent in neonates (4.2%). Enterococcus faecium and E. faecalis had the highest frequency in neonates (6.1% each), with a progressive decline in older age groups. Among Gram-negative bacteria, E. coli and K. pneumoniae isolates showed a significant decrease between the 0–28 days and 13 months–2 years age groups, followed by a notable increase in children over 9 years. Salmonella spp. infections peaked in the 13 months–2 years group (3.1%) [24].
Regarding the significant risk factors for acquiring healthcare-associated infections, including BSIs, the following were identified in the reviewed studies: recent hospitalization (8/19, 42.1% vs. 17/132, 12.9%; p < 0.001), presence of comorbidities (17/19, 89.5% vs. 72/132, 54.5%; p < 0.004) [38], admission to the PICU (OR 2.0), malnutrition (OR 1.6), HIV infection (OR 1.7), “fatal” McCabe score (OR 2.0), comorbid conditions (OR 1.6), use of implanted medical devices (OR 1.9), blood transfusions (OR 2.5), and transfer from another healthcare facility (OR 1.4) [39].
Specifically, multivariate analysis showed that BSIs caused by extended-spectrum beta-lactamase-producing Enterobacteriaceae (ESBL-E) were independently associated with the following risk factors: neonatal period (OR = 11.4), sickle cell anemia (OR = 3.1), malnutrition (OR = 2.0), and mechanical ventilation (OR = 3.5) [40]. Additionally, neutropenia was consistently identified as a significant risk factor for infections with multidrug-resistant (MDR) Gram-negative bacteria in several studies [41-43]. The use of tunneled central venous catheters such as Broviac and Hickman was also associated with a higher risk of CLABSI compared to fully implantable devices such as Port-a-Cath [44]. A study from Qatar reported BSI densities of 3.98 per 1,000 catheter-days for Port-a-Cath and 5.13 for Hickman catheters [45].
The insertion site of the central venous catheter also plays a key role in the development of BSIs. A study conducted in adults demonstrated a significantly higher risk of bacteremia with femoral catheters (24.5%; 100 out of 407) compared to those placed in the internal jugular vein (10.4%; 36 out of 346), with a relative risk of 2.36. Moreover, the average time to infection onset was shorter for femoral catheters (20.11 ± 6.91 days) compared to internal jugular catheters (25.97 ± 6.56 days) [46].
Among children with hemato-oncological conditions, significant risk factors for the development of BSIs included corticosteroid treatment (50.3% vs. 68.4%; p = 0.02), antibiotic therapy (62.7% vs. 77.2%; p = 0.05), chemotherapy (67.3% vs. 84.2%; p = 0.01) in the 30 days preceding BSI onset, neutropenia (21.6% vs. 54.4%; p < 0.001), and mucositis (12.4% vs. 29.8%; p < 0.001) [47]. On the other hand, in children with solid tumors, surgical interventions (7.2% vs. 0%; p = 0.03), bed immobilization (41.8% vs. 15.8%; p < 0.001), and mechanical ventilation (12.4% vs. 1.8%; p = 0.01) in the 72 hours preceding the onset of bacteremia were identified as significant risk factors [48].
Bloodstream infections represent a severe and frequent complication among children who develop HA-BSIs, with mortality rates increasing significantly in immunocompromised patients [49]. A multicenter study conducted in New York, which included 4,500 children, found that the probability of death was nearly six times higher in patients with BSIs compared to those without (95% CI: 3.02–16.00; p < 0.05) [50]. Clinical outcomes were unfavorable, with a crude mortality rate of 41.3% and a mean PICU length of stay of 15 days [51]. Recent studies have reported that mortality rates associated with BSIs range from 21 to 32 deaths per 100,000 population [51, 52], while the one-month post-diagnosis mortality is estimated at 17%–28% for HA-BSIs and 10%–19% for community-acquired BSIs [53, 54]. Higher mortality rates of 40%–50% were observed in studies involving pediatric patients with BSIs admitted to intensive care units [55]. For instance, 45.4% of pediatric patients with BSIs caused by Enterobacteriaceae died, with significantly higher mortality in infections caused by ESBL-positive strains (54.8%) compared to ESBL-negative strains (15.4%) (p < 0.001). Univariate analysis showed that fatal outcomes were more frequent in neonates and younger children, while multivariate analysis identified ESBL production as an independent risk factor for mortality (OR = 2.9; 95% CI: 1.8–7.3; p = 0.001) [40]. The average length of stay (LOS) for patients with BSIs caused by ESBL-positive strains was 22.5 days (95% CI: 18.5–26 days), compared to 12.6 days (95% CI: 9.5–15.8 days) for those with ESBL-negative strains (p < 0.0001) [40]. Children with BSIs and respiratory tract infections (RTIs) had 4.0- and 2.9-fold higher mortality risk, respectively, compared to children with other types of HAIs [18]. A retrospective cohort study in the USA showed that patients with BSIs had a significantly higher crude mortality rate than those without (5% vs. 0.34%; p < 0.001) [56].
In pediatric oncology patients, early (7-day) and late (30-day) mortality rates were 3.8% and 13.8%, respectively. These rates were similar between patients with solid tumors (ST) and those with hematologic malignancies (HM). However, PICU care was significantly more frequent in children with ST than in those with HM (23.5% vs. 10.5%; p = 0.05), while the duration of hospitalization after a BSI episode was significantly longer in children with HM compared to those with ST (median 19 vs. 13 days; p = 0.02) [47]. Unit-stratified outcomes showed a greater impact of HA-BSIs in pediatric intensive care units (PICUs), with a mean attributable LOS of 16.4 days, compared to neonatal ICUs (NICUs), where the mean was 11.4 days. In PICUs, the attributable LOS ranged from 11.4 to 21.1 days, while in NICUs, it varied from 4 to 27.8 days [2]. This trend was also reflected in cumulative mortality rates, which were higher in PICUs (0.13) compared to NICUs (0.08). Furthermore, both the average LOS and mortality rate were significantly higher in patients who developed HAIs, with an LOS of 25 days versus 7 days in patients without HAIs (p < 0.0001) and a mortality rate of 50% versus 27.8% (p < 0.005) [57].
The relationship between total cost and independent variables in PICU patients showed that the median cost was highest for children under two months of age, at €6,903.30. Additionally, there was a significant difference between the median cost of patients with bloodstream infections (€37,356.68) and those with pneumonia (€34,912.96). Costs increased proportionally with the number of HAIs diagnosed; the cost difference between patients with one infection and those with three or four reached €38,202.57. Multivariate analysis revealed that patients with bloodstream infections (p < 0.001) incurred significantly higher costs compared to those without HAIs. The average direct healthcare cost for patients with HA-BSIs ranged between $1,642.16 and $160,804 (in 2019). Moreover, direct costs were estimated at $371,887, which included 2,275 additional hospital days, 2,365 days of antimicrobial therapy, and 3,575 additional laboratory investigations [39].
In Greece, the average LOS and cost attributable to CLABSI in the pediatric and neonatal population were 21 days and €13,727, respectively (Table 1). The high incidence of CLABSI reported in the literature (4.41 infections per 1,000 central line-days) further emphasizes the need for preventive measures. This incidence varies by ICU type, reaching 6.02 in NICUs, 6.09 in PICUs, and 2.78 in Hematology-Oncology units [58].
Table 1. Length of hospital stay and costs of bloodstream infections in children in Greece (58) | ||||
Variable | CLABSI (n = 94) | Non - CLABSI (n = 94) | Difference | 95% IC |
LOS, Overall days1 | 57.1 | 36.6 | 21 | 7.3-34.8 |
By unit |
|
|
|
|
PICU | 52.1 | 33.2 | 19.1 | 5.7-32.6 |
NICU | 75 | 47.8 | 27.8 | 8.7-46.9 |
Hematology-Oncology Unit | 69.8 | 44.5 | 24.8 | 6.8-42.9 |
Bone marrow transplantation unit | 34 | 21.7 | 12.4 | 4.1-20.8 |
Cost, Overall € | 31.302 | 17.788 | 13.727 | 5.758-21.677 |
By unit |
|
|
|
|
PICU | 29.282 | 16.951 | 13.159 | 4.642-21.677 |
NICU | 36.582 | 20.788 | 16.275 | 6.194-26.357 |
Hematology-Oncology Unit | 38.503 | 21.881 | 16.442 | 5.646-27.238 |
Bone marrow transplantation unit | 21.166 | 12.028 | 9.272 | 3.661-14.883 |
Note: CI, Confidence interval; LOS, Length of hospital stay after study enrollment. 1LOS and cost are adjusted for age, gender, hospital, hospitalization unit, LOS prior to study enrollment, CVC outcomes after study enrollment and for propensity score. Propensity score variables include catheter placement, presence of stomy the last 48 h prior to study enrollment, presence of neutropenia and transfusion of blood products the last 14 days prior to study enrollment, LOS in ICU and length of catheter stay prior to study enrollment. €- Euro, the monetary unit and official currency of the European Union. | ||||
Although the incidence of this group of infections is high among pediatric patients, existing evidence in the scientific literature shows that bloodstream infections (BSIs) can be prevented. For example, in one study, during the control period, the rate of central line-associated bloodstream infections (CLABSI) was 7.4. After implementing preventive measures, during the intervention period, this rate significantly decreased to 4.78. In the follow-up period, the downward trend was maintained, reaching 2 [59]. A similar reduction in the incidence of bloodstream infections was observed in another study conducted in a pediatric intensive care unit. During the reference period, the infection rate was 88 per 1000 admissions, and after prevention measures were implemented, it decreased to 41 per 1000 admissions. Most of these infections were associated with the use of central venous catheters (CVCs), and the catheter-related infection rate decreased from 25.2 per 1000 CVC-days to 9.3 per 1000 CVC-days (p < 0.05). These results emphasize the importance of applying effective protocols to reduce CLABSI and improve patient outcomes [60].
A remarkable example of success was recorded in the neonatal services at Nationwide Children’s Hospital, where the CLABSI rate was reduced from 6.0 to 1.43 per 1000 catheter-days in less than two years and then maintained at 0.68 for over five years [61]. Another study conducted in China showed a significant decrease in CLABSI incidence during the COVID-19 pandemic compared to the pre-pandemic period, from 9.4 to 2.2 per 1000 catheter days (P < 0.001) [62]. This downward trend was correlated with several factors, the main ones being improved infection prevention and control measures, with the implementation of stricter hygiene protocols and the use of personal protective equipment; reduced hospital admissions and invasive procedures; closer monitoring of patients with central venous catheters; and limiting access of visitors and auxiliary staff [62].
According to data from the Republic of Moldova, in 2023, 163 cases of healthcare-associated infections (HAIs) were reported in children aged 0 to 17 years. Among these, the following were recorded: surgical site infections – 32 cases (19.6%), infections following therapeutic injections, infusions, or transfusions – 21 cases (12.9%), nosocomial pneumonia due to mechanical ventilation – 106 cases (65%), and urinary tract infections following medical interventions – 4 cases (2.5%). These represented approximately 7.5% of the total reported infections (Figure 2).
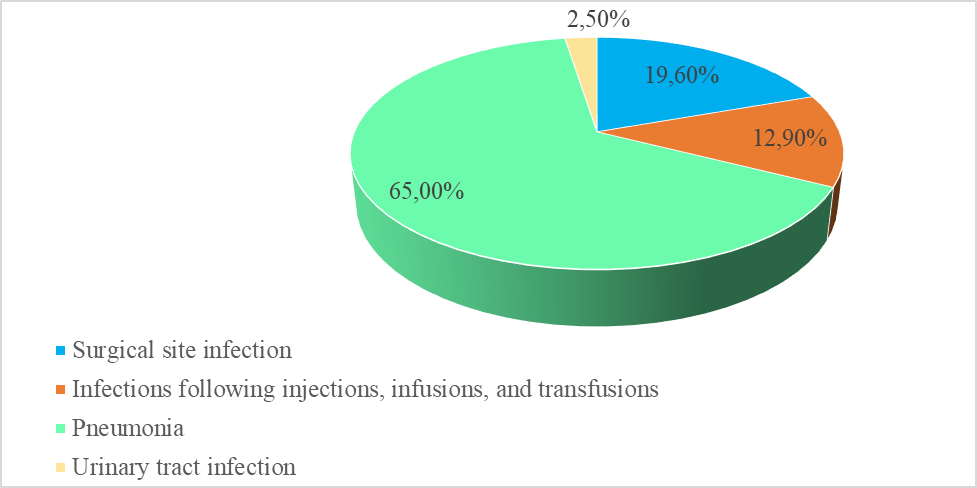 |
Fig. 2 Structure of morbidity due to healthcare-associated infections in children aged 0–17 years, in the Republic of Moldova, 2023. Note: Data are presented as percentages of the total number of reported healthcare-associated infection cases in children aged 0–17 years (n = 163). The figure was developed based on data collected through Statistical Form No. 2, “Report on Certain Infectious and Parasitic Diseases Registered in the Republic of Moldova” for the year 2023, as officially reported by the National Agency for Public Health. Percentages may not sum to 100% due to rounding. |
Data regarding the structure of morbidity due to healthcare-associated infections in newborns in the Republic of Moldova differ from those identified in children aged 0–17 years (Figure 3). Additionally, the number of HAI cases was higher in newborns, emphasizing the biological fragility of this group and the increased exposure to infectious risks from the very first days of life.
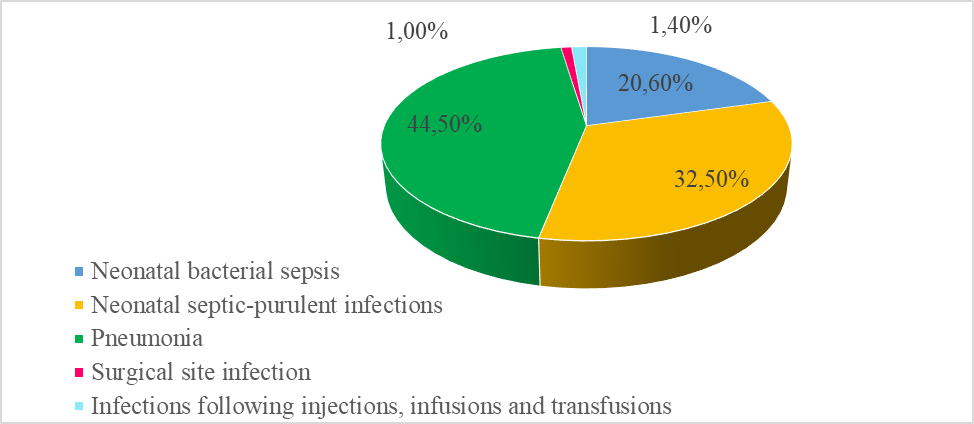 |
Fig. 3 Structure of morbidity due to healthcare-associated infections in newborns, Republic of Moldova, 2023 Note: Data are presented as percentages of the total number of reported healthcare-associated infection cases in newborns (n = 209). The figure was developed based on data collected through Statistical Form No. 2, “Report on Certain Infectious and Parasitic Diseases Registered in the Republic of Moldova” for the year 2023, as officially reported by the National Agency for Public Health. Percentages may not sum to 100% due to rounding. |
Until now, no comprehensive study has been conducted addressing the issue of healthcare-associated infections (HAIs) in children in the Republic of Moldova [6]. However, it is noteworthy that a component of this topic was investigated within the framework of the “First National Point Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use in Hospitals of the Republic of Moldova,” which highlighted that septicemia accounts for 1.2% of all HAIs identified among both adults and children [63].
Discussion
Healthcare-associated bloodstream infections represent a major concern in pediatric care globally, significantly impacting morbidity, mortality, and healthcare system costs. Despite sustained efforts in prevention and control, incidence rates remain high, underscoring the need for the development and implementation of more effective strategies tailored to the pediatric population. Published data on pediatric HA-BSI vary considerably depending on the country, the profile of healthcare facilities, and the year of publication [12, 18, 20].
Epidemiological studies report a high incidence of HA-BSI ranging between 2 and 25 cases per 1,000 central venous catheter days, with higher rates observed in pediatric and neonatal intensive care units [2, 12, 16-18]. Although bloodstream infections represent one of the predominant forms of healthcare-associated infections, the greatest burden is borne by newborns and children under one year of age, accounting for over 50% of all healthcare-associated infections identified in these vulnerable groups. Additionally, children with solid tumors and hematologic-oncologic conditions exhibit increased susceptibility to HA-BSI due to severe immunosuppression induced by chemotherapy, radiotherapy, and immunosuppressive treatments. In these patients, the risk of infection is further amplified by the frequent and prolonged use of central venous catheters [47].
Another critical aspect of the impact of HA-BSI is the prolongation of hospital stays. Studies show that pediatric patients who develop bloodstream infections require longer hospitalizations, averaging approximately 25 days, compared to only 7 days among children without these infections, directly leading to increased treatment costs and prolonged exposure to nosocomial pathogens [2]. Furthermore, each episode of bloodstream infection can add between 10 and 21 additional days to the length of stay, increasing the risk of complications and the need for additional medical resources [2]. It has also been observed that bloodstream infections caused by ESBL-positive strains are associated with a significantly longer average hospital stay compared to those caused by non-ESBL strains [18, 34, 40].
The economic impact of healthcare-associated bloodstream infections is considerable, generating both direct and indirect costs that place significant pressure on healthcare systems. Hospital expenses are significantly higher in patients who develop bloodstream infections compared to those who do not, varying according to the number, severity, and complexity of infections. Total costs can range from 1,642.16 USD to 160,804 USD per patient [39, 58].
Direct costs are mainly related to prolonged hospital stays, the use of broad-spectrum antibiotics, the need for intensive supportive therapies, as well as the necessity for additional laboratory investigations. Beyond direct costs, there is also a significant economic impact on patients' families, reflected in economic losses caused by parents' absence from work during the child's hospitalization [64-66]. Mortality associated with these infections ranges between 15% and 50%, depending on case severity, patient comorbidities, and the type of microorganisms involved. Severe cases, especially in intensive care units and among children with hematologic-oncologic conditions, have higher mortality, with antibiotic-resistant and fungal strains posing additional risk factors [47].
Among the main pathogens involved in healthcare-associated bloodstream infections are Gram-positive bacteria, especially Staphylococcus spp., including coagulase-negative staphylococci, followed by Gram-negative bacteria such as Klebsiella spp., Acinetobacter spp., and Escherichia coli, which in the last decade have played an increasingly significant role in the etiology of HA-BSI [16, 24-26, 30]. Furthermore, there is a notable spread of fungal infections, particularly those caused by Candida spp., which continue to increase and can reach incidences of 20–30 cases per 1,000 catheter-days, with mortality rates ranging from 12% to 41%. Fungal infections are often associated with prolonged use of central venous catheters and antimicrobial treatments, which can disrupt the normal microbial flora and favor fungal proliferation. Increased risk of Candida infections is also associated with factors such as immunosuppression, parenteral nutrition, diabetes, and prolonged hospitalization [5, 31, 32].
Early diagnosis and prompt initiation of treatment are essential in managing HA-BSI, especially since empirical treatment is often started before blood culture results are available due to the urgent need to control infection [24]. However, a significant challenge in treatment is the growing presence of resistant microorganisms such as methicillin-resistant Staphylococcus aureus (MRSA), extended-spectrum beta-lactamase-producing Enterobacteriaceae (ESBL-E), and vancomycin-resistant enterococci, which further complicate therapies [24, 33, 34]. Additionally, a major difficulty in managing HA-BSI is diagnosis, as in approximately 30.9% of cases, the source of infection cannot be identified, either due to inconclusive clinical evaluation (20.8%) or lack of complete medical data (10.1%) [21]. In this context, the rising antimicrobial resistance – especially to beta-lactams and carbapenems – necessitates adopting more precise and personalized therapeutic strategies to limit complications and improve prognosis in pediatric patients [33-35].
Among the main risk factors involved in the development of HA-BSI identified in the analyzed studies are young age, admission to intensive care units, recent hospitalization, use of invasive medical devices, interhospital transfer, malnutrition, presence of comorbidities, HIV infection, and blood transfusion [21,38-40]. Specific factors such as the neonatal period, sickle cell anemia, mechanical ventilation, and neutropenia have been independently associated with an increased risk of acquiring bloodstream infections caused by extended-spectrum beta-lactamase-producing bacteria [18, 27, 40].
Studies show that strict implementation of prevention and control measures can significantly reduce the incidence of nosocomial infections, thereby helping to decrease the costs associated with patient care [61, 67]. For example, it has been estimated that reducing central line-associated bloodstream infections in neonatal units can generate savings of approximately 348,000 USD per year by decreasing hospitalization duration by 84 days [67]. Additionally, it has been found that femoral catheter insertion represents a higher risk for acquiring HA-BSI and requires more careful management. The use of femoral catheters should be limited to strictly necessary situations, and patients must be closely monitored to prevent complications [46].
Conclusions
Healthcare-associated bloodstream infections remain a major public health issue among pediatric patients, with a significant impact on morbidity, mortality, length of hospital stay, and costs. Despite the high prevalence of these infections, successful examples from various studies suggest that bloodstream infections can be prevented. Thus, the implementation of effective strategies – such as strict adherence to hygiene measures, judicious use of invasive medical devices, rational antibiotic use, and continuous case monitoring – can significantly contribute to reducing the incidence of healthcare-associated bloodstream infections. In this context, epidemiological surveillance and the adoption of evidence-based protocols are crucial for improving the quality of medical care and reducing the impact of these infections on the pediatric population.
Competing interests
None declared.
Acknowledgements and funding
The study had no external funding.
Provenance and peer review
Not commissioned, externally peer review.
Author’s ORCID ID
Irina Marga – https://orcid.org/0009-0003-5868-066X
References
Zingg W, Holmes A, Dettenkofer M, Goetting T, Secci F, Clack L, et al. Hospital organisation, management, and structure for prevention of health-care-associated infection: a systematic review and expert consensus. Lancet Infect Dis. 2015;15(2):212-24. doi: 10.1016/S1473-3099(14)70854-0.
Karagiannidou S, Triantafyllou C, Zaoutis TE, Papaevangelou V, Maniadakis N, Kourlaba G. Length of stay, cost, and mortality of healthcare-acquired bloodstream infections in children and neonates: a systematic review and meta-analysis. Infect Control Hosp Epidemiol. 2020;41(3):342-54. doi: 10.1017/ice.2019.353.
World Health Organization. Report on the burden of endemic health care-associated infection worldwide clean care is safer care [Internet]. Geneva: WHO; 2011 [cited 2025 Jun 6]. Available from: https://www.who.int/publications/i/item/report-on-the-burden-of-endemic….
Jansen SJ, van der Hoeven A, van den Akker T, Veenhof M, von Asmuth EGJ, Veldkamp KE, et al. A longitudinal analysis of nosocomial bloodstream infections among preterm neonates. Eur J Clin Microbiol Infect Dis. 2022;41(11):1327-36. doi: 10.1007/s10096-022-04502-8.
Becerra MR, Tantaleán JA, Suárez VJ, Alvarado MC, Candela JL, Urcia FC. Epidemiologic surveillance of nosocomial infections in a Pediatric Intensive Care Unit of a developing country. BMC Pediatr. 2010;10:66. https://doi.org/10.1186/1471-2431-10-66.
Marga I, Paraschiv A. Infecțiile asociate asistenței medicale la copii [Medical-associated infections in children]. Public Health Econ Manag Med (Chisinau). 2024 Oct;(4):41-9. Romanian. https://doi.org/10.52556/2587-3873.2024.4(101).07.
European Centre for Disease Prevention and Control. Healthcare-associated infections acquired in intensive care units. In: ECDC. Annual Epidemiological Report for 2020. Stockholm: ECDC; 2024.
Goto M, Al-Hasan M. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clin Microbiol Infect. 2013 Jun;19(6):501-9. doi: 10.1111/1469-0691.12195.
Cassini A, Plachouras D, Eckmanns T, Abu Sin M, Blank HP, Ducomble T, et al. Burden of six healthcare-associated infections on European population health: estimating incidence-based disability-adjusted life years through a population prevalence-based modelling study. PLoS Med. 2016 Oct 1;13(10):e1002150. doi: 10.1371/journal.pmed.1002150.
Umscheid CA, Mitchell MD, Doshi JA, Agarwal R, Williams K, Brennan PJ. Estimating the proportion of healthcare-associated infections that are reasonably preventable and the related mortality and costs. Infect Control Hosp Epidemiol. 2011 Feb;32(2):101-14. doi: 10.1086/657912.
Campbell AJ, Blyth CC, Hewison CJ, Chen YP, Gough L, Goff Z, et al. Lessons learned from a hospital-wide review of blood stream infections for paediatric central line-associated blood stream infection prevention. J Paediatr Child Health. 2019 Jun 1;55(6):690-4. doi: 10.1111/jpc.14276.
Singhi S, Nallaswamy K. Catheter related blood stream infection in Indian PICUs: several unanswered issues! Indian J Crit Care Med. 2013;17(3):127-8. doi: 10.4103/0972-5229.117035.
European Centre for Disease Prevention and Control; Suetens C, Kärki T, Plachouras D. Point prevalence survey of healthcare-associated infections and antimicrobial use in European acute care hospitals 2022–2023 [Internet]. Stockholm: ECDC; 2024 [cited 2025 Apr 15]. Available from: www.ecdc.europa.eu
Rosenthal VD, Myatra SN, Divatia JV, Biswas S, Shrivastava A, Al-Ruzzieh MA, et al. The impact of COVID-19 on health care–associated infections in intensive care units in low- and middle-income countries: International Nosocomial Infection Control Consortium (INICC) findings. Int J Infect Dis. 2022 May 1;118:83-88. doi: 10.1016/j.ijid.2022.02.041.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi: 10.1136/bmj.n71.
Pereira CAP, Marra AR, Camargo LFA, Pignatari ACC, Sukiennik T, Behar PRP, et al. Nosocomial bloodstream infections in Brazilian pediatric patients: microbiology, epidemiology, and clinical features. PLoS One. 2013 Jul 4;8(7):e68144. doi: 10.1371/journal.pone.0068144.
Zingg W, Hopkins S, Gayet-Ageron A, Holmes A, Sharland M, Suetens C, et al. Healthcare-associated infections in neonates and children in the first European point prevalence survey. Lancet Infect Dis. 2017 Apr;17(4):381-389. doi: 10.1016/S1473-3099(16)30517-5.
Folgori L, Bernaschi P, Piga S, Carletti M, Cunha FP, Lara PHR, et al. Healthcare-associated infections in pediatric and neonatal intensive care units: Impact of underlying risk factors and antimicrobial resistance on 30-day case-fatality in Italy and Brazil. Infect Control Hosp Epidemiol. 2016 Nov 1;37(11):1302-9. doi: 10.1017/ice.2016.185.
Younous S, Nadifiyine D, Yassine A, Mouaffak Y, Sahraoui HE, Sihami A, et al. High rates of nosocomial infections and antimicrobial resistance in a Moroccan PICU: a cause for alarm. IJID Reg. 2024;13:100423. doi: 10.1016/j.ijregi.2024.100423.
Rosenthal VD, Jarvis WR, Jamulitrat S, Silva CP, Ramachandran B, Dueñas L, et al. Socioeconomic impact on device-associated infections in pediatric intensive care units of 16 limited-resource countries: International Nosocomial Infection Consortium findings. Pediatr Crit Care Med. 2012;13(4):399-406. doi: 10.1097/PCC.0b013e318238b260.
Al Saeghi N, Al Thuhli M, Al Hamrashi H, Al Shibli N, Al Wahaibi A, Al Adawi B, et al. Bloodstream infection in children managed at a tertiary hospital in Oman. Sultan Qaboos Univ Med J. 2024;24(4):501-506. doi: 10.18295/squmj.7.2024.044.
Khazaei S, Adabi M, Bashirian S, Shojaeian M, Bathaei SJ, Karami M. Epidemiologic profile of nosocomial infections among paediatric patients in a referral hospital in Hamadan, west of Iran. New Microbes New Infect. 2020 Nov 1;38. doi: 10.1016/j.nmni.2020.100823.
Wang C, Hao W, Yu R, Wang X, Zhang J, Wang B. Analysis of pathogen distribution and its antimicrobial resistance in bloodstream infections in hospitalized children in East China, 2015–2018. Trop Pediatr. 2021;67(1):fmaa077. doi: 10.1093/tropej/fmaa077.
Sader HS, Castanheira M, Streit JM, Carvalhaes CG, Mendes RE. Frequency and antimicrobial susceptibility of bacteria causing bloodstream infections in pediatric patients from United States (US) medical centers (2014–2018): therapeutic options for multidrug-resistant bacteria. Diagn Microbiol Infect Dis. 2020 Oct 1;98(2):115108. doi: 10.1016/j.diagmicrobio.2020.115108.
Paut O, Orliaguet G. Réanimation pédiatrique. Cham: Springer; 2013.
Jordan Garcia I, Esteban Torné E, Bustinza Arriortua A, De Carlos Vicente JC, García Soler P, Concha Torre JA, et al. Trends in nosocomial infections and multidrug-resistant microorganisms in Spanish pediatric intensive care units. Enferm Infecc Microbiol Clin. 2016 May 1;34(5):286-92. doi: 10.1016/j.eimc.2015.07.010.
Kepenekli E, Soysal A, Yalindag-Ozturk N, Ozgur O, Ozcan I, Devrim I, et al. Healthcare-associated infections in pediatric intensive care units in Turkey: a national point-prevalence survey. Jpn J Infect Dis. 2015 Sep 19;68(5):381-6. doi: 10.7883/yoken.JJID.2014.385.
Le NK, Hf W, Vu PD, Khu DTK, Le HT, Hoang BTN, et al. High prevalence of hospital-acquired infections caused by gram-negative carbapenem resistant strains in Vietnamese pediatric ICUs. Medicine (United States). 2016 Jul 1;95(27):e4099. doi: 10.1097/MD.0000000000004099.
Castanheira M, Deshpande LM, Mendes RE, Canton R, Sader HS, Jones RN. Variations in the occurrence of resistance phenotypes and carbapenemase genes among enterobacteriaceae isolates in 20 years of the SENTRY antimicrobial surveillance program. Open Forum Infect Dis. 2019 Mar 15;6(Suppl 1):S23-33. doi: 10.1093/ofid/ofy347.
Flannery DD, Akinboyo IC, Mukhopadhyay S, Tribble AC, Song L, Chen F, et al. Antibiotic susceptibility of Escherichia coli among infants admitted to neonatal intensive care units across the US from 2009 to 2017. JAMA Pediatr. 2021;175(2):168-75. doi: 10.1001/jamapediatrics.2020.4719.
Dramowski A, Cotton MF, Rabie H, Whitelaw A. Trends in paediatric bloodstream infections at a South African referral hospital. BMC Pediatr. 2015 Apr 2;15(1):33. doi: 10.1186/s12887-015-0354-3.
Lipworth S, Vihta KD, Davies T, Wright S, Tabirao M, Chau K, et al. Molecular epidemiology and antimicrobial resistance phenotype of paediatric bloodstream infections caused by Gram-negative bacteria. Commun Med. 2022;2:101. doi: 10.1038/s43856-022-00161-0.
Venturini E, Montagnani C, Benni A, Becciani S, Biermann KP, De Masi S, et al. Central-line associated bloodstream infections in a tertiary care children’s university hospital: a prospective study. BMC Infect Dis. 2016 Dec 1;16(1):725. doi: 10.1186/s12879-016-2061-6.
Stoll BJ, Puopolo KM, Hansen NI, Sánchez PJ, Bell EF, Carlo WA, et al. Early-onset neonatal sepsis 2015 to 2017, the rise of Escherichia coli, and the need for novel prevention strategies. JAMA Pediatr. 2021;175(2):212. doi: 10.1001/jamapediatrics.2020.6111.
Sands K, Carvalho MJ, Portal E, Thomson K, Dyer C, Akpulu C, et al. Characterization of antimicrobial-resistant Gram-negative bacteria that cause neonatal sepsis in seven low- and middle-income countries. Nat Microbiol. 2021 Apr 1;6(4):512-23. doi: 10.1038/s41564-021-00870-7.
Spaulding AB, Watson D, Dreyfus J, Heaton P, Grapentine S, Bendel-Stenzel E, et al. Epidemiology of bloodstream infections in hospitalized children in the United States, 2009–2016. Clin Infect Dis. 2019 Aug 30;69(6):995-1002. doi: 10.1093/cid/ciy1030.
Hussain MS, Basher H, Lone MS, Wani K. Bloodstream infections in pediatric population in a tertiary care hospital. Int J Contemp Med Res. 2019 Feb;6(2). doi:10.21276/ijcmr.2019.6.2.27
Olivier C, Kunneke H, O’Connell N, von Delft E, Wates M, Dramowski A. Healthcare-associated infections in paediatric and neonatal wards: a point prevalence survey at four South African hospitals. S Afr Med J. 2018 May 1;108(5):418-22. doi: 10.7196/SAMJ.2018.v108i5.12862.
Dramowski A, Whitelaw A, Cotton MF. Burden, spectrum, and impact of healthcare-associated infection at a South African children’s hospital. J Hosp Infect. 2016 Dec 1;94(4):364-72. doi: 10.1016/j.jhin.2016.08.022.
Ndir A, Diop A, Faye PM, Cissé MF, Ndoye B, Astagneau P. Epidemiology and burden of bloodstream infections caused by extended-spectrum beta-lactamase producing enterobacteriaceae in a pediatric hospital in Senegal. PLoS One. 2016 Feb 1;11(2):e0143729. doi: 10.1371/journal.pone.0143729.
Kelly MS, Conway M, Wirth KE, Potter-Bynoe G, Billett AL, Sandora TJ. Microbiology and risk factors for central line-associated bloodstream infections among pediatric oncology outpatients: a single institution experience of 41 cases. J Pediatr Hematol Oncol. 2013;35(2):e71-6. doi: 10.1097/MPH.0b013e3182820edd.
Gaur AH, Bundy DG, Werner EJ, Hord JD, Miller MR, Tang L, et al. A prospective, holistic, multicenter approach to tracking and understanding bloodstream infections in pediatric hematology-oncology patients. Infect Control Hosp Epidemiol. 2017 Jun 1;38(6):690-6. doi: 10.1017/ice.2017.57.
Murshed IAS, Zhao L, Zhang W, Yin Y, Li Y, Peng Y, et al. Bloodstream infections in pediatric hematology/oncology patients: a single-center study in Wuhan. Front Cell Infect Microbiol. 2024;14:1480952. doi: 10.3389/fcimb.2024.1480952.
Wagner M, Bonhoeffer J, Erb TO, Glanzmann R, Häcker FM, Paulussen M, et al. Prospective study on central venous line associated bloodstream infections. Arch Dis Child. 2011 Sep;96(9):827-31. doi: 10.1136/adc.2010.208595.
Alsaad T, Qaisuddin M, AlSaad D, Chandra P, AlAbd O, Nasser A, et al. Central line-associated bloodstream infection in pediatric oncology patients in Qatar: a prospective study. J Appl Hematol. 2017;8(2):49-53. doi: 10.4103/joah.joah_13_17.
Hussain M, Nadeem M, Khan A, Rehman K, Mirza A, Rehman M, et al. Bacterial spectrum and antimicrobial pattern of blood stream infections associated with non-tunneled double lumen catheter in hemodialysis. Pak Armed Forces Med J. 2021;71(4):1161-66. https://doi.org/10.51253/pafmj.v71i4.4438.
Skogberg K, Lyytikäinen O, Ollgren J, Nuorti JP, Ruutu P. Population-based burden of bloodstream infections in Finland. Clin Microbiol Infect. 2012;18(6):E170-6. doi: 10.1111/j.1469-0691.2012.03845.x.
Garrido MM, Garrido RQ, Cunha TN, Ehrlich S, Martins IS. Comparison of epidemiological, clinical and microbiological characteristics of bloodstream infection in children with solid tumours and haematological malignancies. Epidemiol Infect. 2019 Nov 8;147:e298. doi: 10.1017/S0950268819001845.
Ammann RA, Laws HJ, Schrey D, Ehlert K, Moser O, Dilloo D, et al. Bloodstream infection in paediatric cancer centres - leukaemia and relapsed malignancies are independent risk factors. Eur J Pediatr. 2015 May 1;174(5):675-86. doi: 10.1007/s00431-015-2525-5.
Thurman CB, Abbott M, Liu J, Larson E. Risk for health care–associated bloodstream infections in pediatric oncology patients with various malignancies. J Pediatr Oncol Nurs. 2017 May 1;34(3):196-202. doi: 10.1177/1043454216680596.
Ramsunder P, Appel I, Dramowski A. Epidemiology of healthcare-associated bloodstream infections in the paediatric intensive care unit 2021 [Internet]. Stellenbosch: Stellenbosch University; 2021 [cited 2025 May 26]. Available from: https://scholar.sun.ac.za/server/api/core/bitstreams/aebd45cd-563a-423f…
Mehl A, Åsvold BO, Kümmel A, Lydersen S, Paulsen J, Haugan I, et al. Trends in antimicrobial resistance and empiric antibiotic therapy of bloodstream infections at a general hospital in Mid-Norway: a prospective observational study. BMC Infect Dis. 2017 Feb 2;17(1):116. doi: 10.1186/s12879-017-2210-6..
Abubakar U, Amir O, Rodríguez-Baño J. Healthcare-associated infections in Africa: a systematic review and meta-analysis of point prevalence studies. J Pharm Policy Pract. 2022;15(1):99. doi: 10.1186/s40545-022-00500-5.
Holmbom M, Giske CG, Fredrikson M, Balkhed ÅÖ, Claesson C, Nilsson LE, et al. 14-year survey in a Swedish county reveals a pronounced increase in bloodstream infections (BSI). Comorbidity - an independent risk factor for both BSI and mortality. PLoS One. 2016 Nov 1;11(11):e0166527. doi: 10.1371/journal.pone.0166527.
Prowle JR, Echeverri JE, Ligabo EV, Sherry N, Taori GC, Crozier TM, et al. Acquired bloodstream infection in the intensive care unit: incidence and attributable mortality. Crit Care. 2011 Mar 21;15(2):R100. doi: 10.1186/cc10114.
Jin L, Zhao C, Li H, Wang R, Wang Q, Wang H. Clinical profile, prognostic factors, and outcome prediction in hospitalized patients with bloodstream infection: results from a 10-year prospective multicenter study. Front Med (Lausanne). 2021 May 20;8:629671. doi: 10.3389/fmed.2021.629671.
Ekubu Otim M, Nawaz Khan H, Grima S, Naylor NR, Yamashita K, Iwami M, et al. Code-sharing in cost-of-illness calculations: an application to antibiotic-resistant bloodstream infections cost-of-illness for antibiotic resistance. Front Public Health. 2020 Nov 27;8:562427. doi: 10.3389/fpubh.2020.562427.
Karagiannidou S, Zaoutis T, Maniadakis N, Papaevangelou V, Kourlaba G. Attributable length of stay and cost for pediatric and neonatal central line-associated bloodstream infections in Greece. J Infect Public Health. 2019 May 1;12(3):372-9. doi: 10.1016/j.jiph.2018.12.004.
Wassef MA, Ghaith DM, Hussien MM, El-Shazly MA, Yousef RHA. Bundle care approach to reduce device-associated infections in post-living-donor-liver transplantation in a tertiary care hospital, Egypt. BMC Infect Dis. 2024 Dec 1;24(1):674. doi: 10.1186/s12879-024-09525-4.
Ng YY, Abdel-Latif MEA, Gan CS, Siham A, Zainol H, Lum LCS. Impact of infection control training for interns on PICU-acquired bloodstream infections in a middle-income country. Singapore Med J. 2015 Sep 1;56(9):506-12. doi: 10.11622/smedj.2015135.
Shepherd EG, Kelly TJ, Vinsel JA, Cunningham DJ, Keels E, Beauseau W, et al. Significant reduction of central-line associated bloodstream infections in a network of diverse neonatal nurseries. J Pediatr. 2015 Jul 1;167(1):41-46.e3. doi: 10.1016/j.jpeds.2015.03.046.
Huang H, Wu K, Chen H, Wang J, Chen L, Lai Z, et al. The impact of the COVID-19 pandemic on nosocomial infections: a retrospective analysis in a tertiary maternal and child healthcare hospital. Front Public Health. 2023;11:1132323. doi: 10.3389/fpubh.2023.1132323.
Busuioc E, Caterinciuc N. Primul studiu național de prevalență de moment a infecțiilor asociate asistenței medicale și a consumului antimicrobienelor în spitalele din Republica Moldova [First national point prevalence survey of healthcare-associated infections and antimicrobial use in acute care hospitals in the Republic of Moldova]. One Health Risk Manag. 2022;3(1):21-8. Romanian. doi: 10.38045/ohrm.2021.4.05.
Friedman C. The costs of healthcare-associated infections. In: IFIC Basic Concepts of Infection Control. 3rd edition. Portadown (UK): IFIC; 2016 [cited 2025 May 29]. Available from: https://www.theific.org/wp-content/uploads/2016/04/CostsCh29.pdf
Leoncio JM, de Almeida VF, Ferrari RAP, Capobiango JD, Kerbauy G, Tacla MTGM. Impact of healthcare-associated infections on the hospitalization costs of children. Rev Esc Enferm USP. 2019;53:e03486. doi: 10.1590/S1980-220X2018016303486.
De Angelis G, Murthy A, Beyersmann J, Harbarth S. Estimating the impact of healthcare-associated infections on length of stay and costs. Clin Microbiol Infect. 2010 Dec 1;16(12):1729-35. doi: 10.1111/j.1469-0691.2010.03332.x.
Ceballos K, Waterman K, Hulett T, Makic MBF. Nurse-driven quality improvement interventions to reduce hospital-acquired infection in the NICU. Adv Neonatal Care. 2013 Jun;13(3):154-63. doi: 10.1097/ANC.0b013e318285fe70.