

Introduction
The focal disease is a pathological condition characterized by a wide variety of functional disorders and organic tissue alterations, due to chronic foci of infection, from which various microbes, microbial toxins, toxic products of septic tissue disintegration, and endo- and exogenous allergens are disseminated in the body via the blood, nervous system, or digestive tract, generating a vast array of dysfunctional and lesional manifestations [1]. Local infection combines particular features and emphasizes the main aspects, such as clinical manifestations, active or latent evolutionary character, and the existence of an antigenic tissue concentration of the type of a focus. The range of reactions caused by a microbial agent includes both significant general reactions and local changes related to the presence of the pathogen. Thus, we are talking about localized, circumscribed inflammatory reactions – “concentrated reactions” – in which, due to the maximum intensity of microbial aggression and tissue response, we can speak of a center, a nucleus, or, in well-established terminology, a focus of the infectious process [2]. “The mouth is probably the dirtiest place in the human body,” noted Steve Kerrigan, a researcher at the Royal College of Surgeons of Ireland [3].
Illustrious scientists, doctors, and statistical consultants from many countries have demonstrated, through a series of clinical observations and statistics collected over the years, the importance, relevance, and topicality of this condition, presenting major values in terms of both prevalence and incidence. Focal infection appears as a disease of the whole organism, in which there is a chronic primary focus with latent evolution, unnoticed by the patient, and secondary lesions at a distance, which manifest differently. The term focal, in the clinical sense, refers to the presence in the body of an infectious process that is more active in a certain region [4-14].
According to the percentage distribution, 90% of the foci of the body are located in the cephalic region, and 10% in the rest of the body. Research has shown that, on the list of foci of infection, those in the oral cavity are in first place, with 93% of the active foci caused by teeth and their pathologies [15-18] (Table 1).
Table 1. Location of infection outbreaks expressed as a percentage (%) | |||
Extracephalic foci | 10% | Cephalic outbreaks | 90% |
Adnexites | 2-7% | Dento-periodontal outbreaks | 72% |
Bronchi | 0.8% | Tonsillitis | 18% |
Intestine | 0.5% | Sinus foci | <18% |
Extrahepatic bile ducts | 0.5% | Middle ear | <18% |
Note: Focal infections occur predominantly in the area of the stomatognathic apparatus. | |||
Important clinical criteria that mark this fundamental difference of odonto-periodontal focal infection include the profile of local inflammation, the level of the tissue hypersensitivity process, the level of microbial load in the focus, and, no less importantly, the reactivity of the organism.
The anatomical features of the tooth create particularly favorable conditions for chronic, latent infections. The infectious process develops in tissues that do not have the possibility of recovery (enamel, dentin) and in locations (root canal) inaccessible to the body's antimicrobial defense mechanisms [1, 13, 15, 16].
In turn, the oral mucosa forms a non-specific (mechanical) defense zone. Thus, a complex barrier is created, consisting of local structures and biological factors that regulate local permeability to bacteria, fungi, viruses, and toxins. However, this physiological barrier is fragile and, under certain pathological conditions, becomes permeable, serving as an entrance gate to the interior of the body [19]. Studying and critically analyzing the specialized literature, from a historical point of view, it is observed that focal disease, with foci of infection at the level of the teeth, marginal periodontium, and tissues of the oral cavity (such as the mucosa, salivary glands, etc.), has been researched since ancient times. The first deductions regarding focal disease, on the relationship between dental infections and some pathological manifestations of the human body, date back several millennia. The Ebers Papyrus described the disappearance of some organic suffering after the extraction of affected teeth. The Nineveh cuneiform manuscript of 650 BCE mentions a cure for joint pain in King Anapper Essa, also after extraction of affected teeth. A cuneiform inscription on a stone found in Nineveh has been deciphered, showing that the pain in the limbs of the Assyrian king Sardanapalus ceased only after, on the advice of his court physician Araa Nana, he extracted all his teeth [1].
The first communications on the correlation of dental diseases with other pathological manifestations in the body were described in 1900 by Steffel. As early as the ninth century AD, an Arab physician wrote that, “the mouth is only a part of the human body, and what happens to it happens to the whole body”. In 1828, Kocher drew attention to the pathogenic relationship of the dental system with the rest of the human body, describing the connection of nervous and rheumatic diseases with dental diseases. At the end of the 19th century, certain theories were developed, claiming that, following the extraction of teeth with a focus of infection, a cure for general diseases could occur. In 1906, Possler drew attention to the cause-and-effect relationship between chronic dental diseases and remote diseases. Later, at the beginning of the 20th century, “focus disease” was discovered. The theory of “focal infection” was introduced into pathology by Billings in 1912 [20].
Experimental research undertaken by Roșenow, Berger, Hateganu, Goia I., and Moga (1934) showed that focal disease is a disease of the whole organism, comprising 2 pathological entities: a) chronic foci of infection with slow oligo- or asymptomatic evolution, which represent the primary manifestation; b) dysfunctional or lesional manifestations at a distance, with rich and varied symptomatology, which represent the secondary determinations. This framework outlines 5 etiopathogenic theories: microbial etiopathogenic, which considers focal disease as an “attenuated septicemia” due to the migration of microorganisms from the focus via the blood and lymph, and their fixation on organs and tissues; allergic, which states that microbes entering the body cause a change in reactivity with the production of hyperergic antibodies (Ab); toxic, which supports the idea that toxins from the focus migrate through the endo- and perineural lymph, producing irritation of nerve centers and nerve cells; vascular, in which the focus of chronic irritation acts on the central and peripheral vegetative nervous system, determining the response of the vessels through changes in tone: ischemia or vasodilation; and the theory of adaptation syndrome, which regards focal disease as an excessive defense reaction of the body, with the adaptation syndrome being the totality of non-specific manifestations of the body's defense as a result of the action of harmful agents of any nature. According to these theories, the main factors in the dissemination of the infection are decreased body resistance, exacerbation of microbial virulence, tissue hyperemia, and loco-regional trauma [1].
The delegation of the German Medical Association conducted scientific studies and demonstrated that there are interactions between teeth and organs of the human body. Through electropuncture, the relationship between teeth or groups of teeth and organs of the human body was demonstrated for the first time. Thus, some dental diseases can signal organic dysfunctions, and the disease of a tooth corresponding to a certain organ can affect that organ: the incisors are related to the urinary system and can generate chronic infections of the urinary bladder; the canines with the liver, gallbladder, eyes, and stomach; the upper premolars with the large intestine and lungs; the lower premolars with the lungs and spleen (t. 34, 35), and with the lungs and pancreas (t. 44, 45); the upper premolars with the lungs and large intestine; the upper molars (t. 16, 17) with the thyroid, stomach, and pancreas, and (t. 26, 27) with the spleen; the lower molars with the stomach and intestines, the immune system, the maxillary sinus, and the thoracic spine; and the wisdom teeth with the heart and small intestine. To the same extent, there are relationships between teeth and the spine [21].
From the above, we can state that a chronic infection localized in a focus–an organ such as the tonsils, teeth, sinuses, bronchi, or kidneys–is delimited by a fibro-connective membrane, which represents a barrier but is imperfect under certain conditions. With increased aggressiveness of microorganisms, decreased body resistance, exacerbation of microbial virulence, or loco-regional trauma of the oral mucosa, microbes and their toxins can “migrate and infiltrate” via the blood and lymphatic pathways away from the initial focus of infection and stop in another healthy organ, which, in turn, will be affected [22].
Thus, chronic infections in the oral cavity can cause true organic diseases, grouped by Veil under the term “vegetative alarm symptomatology”, which includes fatigue, morning sickness without explainable causes, memory disorders, unexplained nervous irritation, adynamia, tachycardia without organic substrate, episodic or prolonged depressive states, intermittent subfibrillations during the day, chills, long-lasting fever, insomnia, headache, myalgias, arthralgias, and loss of appetite. It is important to note that the dentist is obliged to detect primary infection foci based on clinical, radiological, and, if necessary, laboratory signs, thus establishing a correct diagnosis, after which they remove or treat the foci. Establishing the link between the infection foci and the secondary disease is not only the dentist's task; interdisciplinary collaboration is necessary to prevent the development of the actual outbreak disease [23].
The purpose of the study is to highlight the role of foci of odontogenic infection in the onset and evolution of focal disease.
Material and methods
The present study is a clinical-observational and microbiological study and included 87 patients (with informed consent) with foci of odontogenic infection, classified according to the frequency of pathologies encountered and the virulence of microbial pathogens as follows: with periodontal disease - 35 patients (gingivitis - 11 patients and 24 patients with different stages of periodontitis); with endodontic pathologies - 27 patients (pulpitis - 5 patients and periapical/periodontitis (Pt) - 22 patients); with dental caries of varying severity - 19 patients; and 6 patients with pathologies of the oral mucosa. The patients were selected and examined clinically and paraclinically (radiographically - RVG and OPG) (Figure 1). In patients with periodontal disease, laboratory examinations were performed, including hemogram, leukogram, and microbiological examination of periodontal pockets (PPr) using the polymerase chain reaction (PCR) method (Table 2).
 |
Fig. 1 Severe periodontitis, stage IV, Grade C, and chronic granulomatous apical periodontitis Note: Intraoral clinical and radiographic appearance. |
Table 2. Microbiological profile of a patient with severe periodontitis | |||
Name of the microorganism | Result | Units of measurement | Reference values |
Total mass of bacteria | 8.5 | Ig | <6.5 |
Actinobacillus actinomycetemcomitans | not detected | Ig | <4.0 |
Porphyromonas gingivalis | 8.0 | Ig | <5.0 |
Prevotella intermedia | 6.6 | Ig | <4.5 |
Tannerella forsythensis | 6.9 | Ig | <5.0 |
Treponema denticola | 7.2 | Ig | <3.5 |
Candida albicans | not detected | Ig | <4.5 |
Note: Microbiocenosis – patient's laboratory medical bulletin. | |||
According to the data in Table 2, a high microbial load with periodontopathic agents is observed, the proteolytic enzymes of which are among the most important virulence factors, and their dissemination throughout the human body is a major risk factor in the onset of focal disease. Even if periodontopathic bacteria are only momentarily present in tissues, once the germs, their virulence factors, and/or inflammatory mediators reach distant organs, they can cause similar inflammatory reactions in the new environment, thus leading to tissue diseases or focal disease. Therefore, periodontal disease/periodontitis has a direct and reciprocal link to the development of systemic diseases such as cancer (including oral cancer), diabetes mellitus, cardiovascular diseases, and neurological pathologies, especially the neurodegenerative disease known as Alzheimer's disease [24].
Considering that the present study was largely a clinical-observational one, the patients were evaluated according to the Veil criteria of “vegetative alarm symptomatology”. During patient examination and clinical symptom assessment, 8 of the 14 Veil criteria were used, specifically those to which patients could easily respond at the examination stage and after the removal/treatment of the foci of infection (Table 3).
Table 3. Evaluation of Veil criteria in patients with foci of odontogenic infection at presentation (presence of symptoms and number of patients) | ||||||||
Pathology/criteria | Fatigue without cause | Memory disorders | Nervous irritation without explanation | Adynamia | Depressive states, episodic or prolonged | Disorders | Arthralgia | Loss of appetite |
Dental caries | - | - | - | - | - | - | ± (3) | - |
Endodontic pathologies (P, Pt) | + (18) | - | ± (10) | ± (2) | ± (13) | + (21) | + (16) | - |
Periodontal disease (gingivitis/periodontitis) | + (27) | + (29) | + (19) | ± (11) | + (22) | + (17) | + (14) | ± (9) |
Pathologies of the oral mucosa | ± (2) | - | + (6) | ± (1) | ± (3) | + (6) | - | + (5) |
Note: Representation of clinical symptoms based on the evaluation at the examination stage - the criteria are indicated in the table. | ||||||||
Based on the data in Table 3, we note that dental caries is one of the most widespread dental diseases; however, the presence of “vegetative alarm symptoms” is not critical, except for sporadic symptoms (in cases of multiple or decompensated caries), because the body's reactivity compensates. In contrast, in endodontic pathologies (chronic pulpitis, apical periodontitis), especially closed forms, residual cysts, etc., these symptoms are much more pronounced. Closed infections are more dangerous than suppurative ones, which have a drainage pathway (Figure 2). Periapical foci are the most frequent complications of dental caries, being represented by chronic pulpitis and chronic fibrous or granulomatous apical periodontitis, residual cysts, etc. [13].
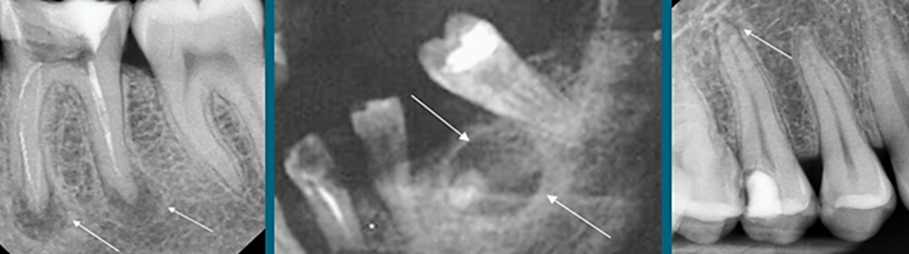 |
Fig. 2 Chronic closed odontogenic foci Note: Radiographic appearance of the periapical lesion and residual cyst (personal case study – S. Ciobanu)[4, 6] |
At the same time, periodontal infection foci, having periodic escape routes, in terms of interaction with the entire organism, exert a much greater influence by affecting all periodontal tissues and by the presence of predominantly anaerobic (Gram-) periodontopathic microorganisms with increased virulence; thus, the expression of “alarm symptoms” is more pronounced (Table 3). A similar situation occurs in the case of foci located in the oral mucosa, taking into account the advanced absorption capacity of the oral mucosa. An important irritating action is also exerted by toxic environmental factors (toxic gases, dust, cigarette smoke, etc.). The virulence of germs is locally exacerbated due to particular anatomical conditions, episodic insufficiency of local non-specific defense factors, and local circulatory disorders that reduce the contribution of general defense mechanisms. Serum concentrations of IgG, IgA, and IgM are lower in smokers, thus disrupting the body's defenses, and macrophages lose part of their adhesion and phagocytic capacity. Viral infections may also play a role in the onset and maintenance of autoimmune diseases [21].
All patients in the study underwent treatment to eliminate or remove foci of infection, according to protocols specific to the pathologies studied, as follows: treatment of dental caries, endodontic treatments, and complex treatment of periodontal disease and lesions of the oral mucosa, thus interrupting the spread of infection throughout the body.
Results
Along the course of treatment and especially at the end of the treatment of the studied pathologies, the patients were evaluated according to the same eight Veil criteria. Thus, through clinical observations, it was found that with the removal of the foci of infection, the “vegetative alarm symptoms” began to disappear, some even very quickly, such as causeless fatigue. At the same time, symptoms present for a longer period of time, such as long-term depressive states and memory disorders in patients with periodontal disease, in this case severe periodontitis with a major microbial load and lesions of the oral mucosa, diminished more slowly, over a period of up to 1-3 months (Table 4).
Table 4. Evaluation of Veil criteria after removal of odontogenic infection foci (presence of symptoms and number of patients) | ||||||||
Pathology/criteria | Fatigue without cause | Memory disorders | Nervous irritation without explanation | Adynamia | Depressive states, episodic or prolonged | Disorders | Arthralgia | Loss of appetite |
Dental caries | - | - | - | - | - | - | - | - |
Endodontic pathologies (P, Pt) | - | - | + (1) | - | - | + (2) | + (1) | - |
Periodontal disease (gingivitis/periodontitis) | - | - | - | - | + (2) | - | + (4) | - |
Pathologies of the oral mucosa | - | - | - | - | - | - | - | - |
Note: Representation of clinical symptomatology based on the evaluation of Veil criteria post-treatment – personal results [4]. | ||||||||
Therefore, by analyzing the symptomatology of patients with odontogenic foci, we find that the “vegetative alarm symptoms” subside significantly, which once again confirms that microbial germs, their virulence factors, and/or inflammatory mediators– such as IL-1, IL-6, IL-8, and TNF–are produced locally in odontogenic foci (periodontal pockets (PPr), periapical lesions, etc.), causing distant systemic inflammation, and that their removal restores the biological balance of the entire organism (Table 4). The 100% disappearance of symptoms in the case of carious lesions and oral mucosal pathologies demonstrates the direct relationship between the foci of infection and the patient's general health. In relation to periodontal disease and periapical lesions, over 90% of symptoms subsided; the clinical signs that were maintained are related to the increased bacterial load and the virulence of pathogens.
Discussion
The oral cavity has a complex microbial ecology, which represents an ideal habitat for the growth and reproduction of many microorganisms, ranging from bacteria to fungi, molds, and viruses. There are many opinions among researchers according to which focal disease is a condition caused by the simultaneous action of several factors that contribute to the decrease in the reactivity of the organism in general and at the level of the oral cavity in particular. According to the data of Ghicavîi et al. (2002), damage to an organ or a system depends largely on constitutional factors, individual receptivity, and the general condition of the organism [25]. An important role is also played by general conditions, and dysfunctional lesional manifestations, which in turn depend on the aggressiveness of the chronic focus, the number of foci, their content, the virulence of microorganisms, etc. The onset of clinical manifestations of systemic disease, conditioned by the presence of odontogenic foci, is diverse and produces major changes in the immunological state of the entire organism. Thus, it is appropriate to place the qualification of an “infection focus” in a context corresponding to the current level of knowledge of local and general pathophysiological mechanisms, as well as immunological and microbiological processes. In this context, the idea of dividing morpho-clinical entities into active focal infections and latent focal infections appears of interest. The available literature suggests that the oral microbiota originating from odontogenic foci plays a significant role in the onset of focal disease, from the moment inflammatory mediators enter the bloodstream and exert a direct impact on distant tissues and organs, as shown by Miklossy et al. (2016) [24].
The study by Dominy et al. (2019) showed that over 90% of brain samples taken from patients with Alzheimer's disease contained gingipains as the most significant virulence factors. P. gingivalis or its virulence factors were repeatedly administered to animal subjects, which led to cognitive decline and an increase in pro-inflammatory mediators (β-amyloid) in their brains. Periodontal disease causes the spread of bacteria or toxins to the brain through peripheral nerves, with the trigeminal nerve being the main access point [26].
Solving dental problems is necessary in the presence of diseases of major organs. Thus, timely treatment, under the strict guidance of a specialist, has beneficial effects on the entire body, not only local effects in the oral cavity.
Conclusions
The identification, evaluation, and removal of foci of odontogenic infection have an important role in aggravating already existing systemic conditions, thus triggering focal disease. The role of the dentist in the prophylaxis of focal disease is a primary one in the detection and elimination of foci of odontogenic infections. In the prophylaxis of focal disease, doctor-patient cooperation is very important, and no less important is collaboration with general medicine specialists.
Competing interests
None declared.
Authors’ contribution
All authors contributed to the conduct of this research.
Informed consent for publication
Obtained.
Ethics approval
The clinical cases in this study were selected from the list of patients treated in the dental clinic, based on informed consent and confirmed consent by signature in the medical record. Thus, approval of the Bioethics Committee was not required.
Acknowledgements and funding
No external funding.
Provenance and peer review
Not commissioned; externally peer-reviewed.
Authors’ ORCID IDs
Sergiu Ciobanu – https://orcid.org/0000-0002-7955-545X
Diana Marcu – https://orcid.org/0000-0002-3844-9175
Ion Roman – https://orcid.org/0009-0006-2241-6973
Olesea Musteață – https://orcid.org/0000-0002-2368-4930
References
Goia I. L’infection de foyer [Focal infection]. 2nd ed. Bucharest; 1946. French.
Maier N. Observații personale privind noțiunea de „focar” în procesele infecțioase [Personal observations concerning the notion of “focal” infection]. DermatoVenerol (Bucharest). 2011;56:131-138. Romanian, English.
Society for General Microbiology. Bleeding gums linked to heart disease. 2008 Sep 11. In: ScienceDaily [Internet]. Encinitas: ScienceDaily; 1995-2025 [cited 2925 Oct 12]. Avilable from: https://www.sciencedaily.com/releases/2008/09/080910210523.htm
Ciobanu S. Tratamentul complex în reabilitarea pacienţilor cu parodontite marginale cronice [Complex treatment in the rehabilitation of patients with chronic marginal periodontitis]. Chişinău: [s. n.]; 2012. 183 p. Romanian.
Dumitriu H, Dumitriu S, Dumitriu A. Parodontologie [Periodontology]. 4th ed. Bucharest: Viaţa Medicală Românească; 2006. p. 40-59. Romanian.
Fala V, Lacusta V, Ciobanu S, Bordeniuc G. Impact of periodontitis on the ECG dispersion mapping of the myocardial tissues. Stomatol Edu J. 2019;6(3):167-175. https://doi.org/10.25241/STOMAEDUJ.2019.6(3).ART.1.
Maier N. O reconsiderare a conceptului de ”infecție de focar” în patologia cutanată [A reconsideration of the concept of “focal infection” in skin pathology]. In: [National Dermatology Conference; 1997 Nov 6-8; Cluj-Napoca, Romania: Abstracts]. Cluj-Napoca; 1997. p. 10. Romanian.
Ichim L, Ghiorghe A, Nunchievici I, Lăcătuşu Ș. Studii privind rolul unor focare de infecție odonto-parodontale în apariția sau agravarea unor boli sistemice [The studies of dental focal infection to appearancing and aggravating the sistemic diseases]. Med Stomatol (Chisinau). 2008;(3):28-30. Romanian.
Hunter W. The role of sepsis and antisepsis in medicine and the importance of oral sepsis as its chief cause. Dent Regist. 1911;65(12):577-611.
Morari I, Şteţiu A, Silivăşan V. Diagnosticul bolii parodontale. Principii generale de abordare [Diagnosis of periodontal disease. General principles of approach]. Dento Medica. 2002;2-3. Romanian.
Olinescu R. Metode biochimice de laborator clinic [Clinical laboratory biochemical methods]. Bucharest: Cerma; 2001. Romanian.
Pallasch TJ, Wahl MJ. The focal infection theory: appraisal and reappraisal. J Calif Dent Assoc. 2000;28(3):194-201.
Roman A. Parodontopatii asociate factorilor sistemici: implicații terapeutice [Periodontopathies associated with systemic factors: therapeutic implications]. Cluj-Napoca: Todesco; 2001. Romanian.
Săceleanu A. Boala dentară de focar. Etiopatogenie şi diagnostic [Focal dental disease. Etiopathogenesis and diagnosis]. Acta Med Transilvanica. 2014;2(3):142-145. Romanian.
Bodrug V. Flora microbiană a canalelor radiculare la pacienţii cu periodontită apicală de etiologie infecţioasă [Microbial flora of root canals in patients with apical periodontitis of infectious etiology]. In: Current issues of dentistry: Proceedings of the 11th National Congress of Dentists of the Republic of Moldova; 2001 Oct 9-10; Chisinau. Romanian.
Borovski E, editor. Stomatologie terapeutica [Therapeutic dentistry]. Chisinau: Lumina; 1990. p. 286-291. Romanian.
Lungu I, Duma I, Pop A, et al. Parodontologie şi boala de focar [Periodontology and focal disease]. Cluj-Napoca: [s. n.]; 1995. 124 p. Romanian.
Toader C, Toader M, Mitea G, et al. Conceptul de infecție de focar amigdalian [The concept of tonsillar focal infection]. Rom J Med Pract. 2015;10(3):269-272. Romanian.
Marcu D. Viziuni privind sensibilitatea levurilor genului Candida la preparatele antimicotice aplicate în tratamentul parodontitelor cronice generalizate [Perspectives on the sensitivity of Candida genus yeasts to antifungal agents applied in the treatment of chronic generalized periodontitis]. Bull Acad Sci Mold. Med Sci. 2012;(2):103-108. Romanian.
Spielman, AI. History of oral diagnosis, medicine, pathology and radiology. In: Illustrated encyclopedia of the history of dentistry [Internet]. 2023 [cited 2025 Sep 12]. Available from: https://historyofdentistryandmedicine.com/history-of-oral-diagnosis-medicine-pathology-and-radiology/
Matsuo T, Kakita S, Honda H, Mori S, Araki K, Mitsunari K, Ohba K, Mochizuki Y, Imamura R. Relationship between tooth loss due to chronic periodontitis and lower urinary tract symptoms. Medicina (Kaunas). 2024;60(11):1829. doi: 10.3390/medicina60111829.
Marcu D, Ababii V. Conceptul de pre-cancer oral = The concept of oral pre-cancer. Med Stomatol (Chisinau). 2020;(2):77-84. Romanian, English.
Li X, Kolltveit KM, Tronstad L, Olsen I. Systemic diseases caused by oral infection. Clin Microbiol Rev. 2000;13(4):547-58. doi: 10.1128/CMR.13.4.547.
Miklossy J, McGeer PL. Common mechanisms involved in Alzheimer's disease and type 2 diabetes: a key role of chronic bacterial infection and inflammation. Aging. 2016;8(4):575-88. https://doi.org/10.18632/aging.100921.
Ghicavîi V, Sîrbu S, Bacinschi N, Scerbatiuc D. Farmacoterapia afecțiunilor stomatologice [Pharmacotherapy of dental disorders]. 2nd ed. Chișinău: [s. n.]; 2002. 628 p. Romanian.
Dominy SS, Lynch C, Ermini F, et al. Porphyromonas gingivalis in Alzheimer's disease brains: evidence for disease causation and treatment with small‐molecule inhibitors. Sci Adv. 2019;5(1):eaau3333. doi: 10.1126/sciadv.aau3333.