
Introduction
Education-based interventions should be evaluated with a focus on promoting behaviors related to the identification, prevention, and management of risk factors, leading to an effective reduction in the incidence of osteoporosis.
Osteoporosis represents a major public health issue globally, particularly affecting the elderly population. It is characterized by a reduction in bone mass and the deterioration of bone tissue structure, which increases the risk of fractures. According to the World Health Organization, osteoporosis affects millions of people worldwide, and its incidence is rising due to the aging population [1]. The risk factors for osteoporosis are numerous and include age, sex, genetic factors, lifestyle, diet, and exposure to certain toxic substances or environmental conditions [2, 3].
Preventing osteoporosis involves a comprehensive approach to managing risk factors. Identifying and managing these risk factors are essential for the prevention and control of the disease. They can include genetic elements as well as environmental and lifestyle factors. Adequate intake of calcium and vitamin D, a healthy diet, and consuming drinking water with an appropriate mineral salt composition are essential for maintaining bone health. Adopting a healthy lifestyle, avoiding smoking, and limiting alcohol consumption are important for preventing osteoporosis.
In the context of osteoporosis prevention and management, the hygienic evaluation of the impact of risk factors plays a crucial role. Developing specific tools that allow for the identification and estimation of the influence of modifiable factors on the development of osteoporosis is an important step in early intervention for at-risk individuals. The importance of such a tool is supported by the need for precise data to guide preventive interventions and to optimize public health strategies aimed at reducing the incidence of osteoporosis. Previous studies have demonstrated that using questionnaires to assess osteoporosis risk can significantly contribute to early risk identification, improve clinical outcomes, and reduce the disease burden [4-7].
The present study focuses on the development and validation of a questionnaire designed for the hygienic assessment of the impact of risk factors, especially modifiable ones, on morbidity due to osteoporosis. This research aims to provide a useful tool for public health professionals and researchers, thereby facilitating the more effective identification and management of risks associated with osteoporosis.
Material and methods
To achieve the proposed aim, both secondary and primary studies were conducted as part of this research.
Secondary research. The narrative synthesis involved collecting information from international open-access databases – PubMed and Google Scholar – using the following keywords: “osteoporosis”, “drinking water”, “mineral composition of drinking water”, “risk factors”, “modifiable factors”, “non-modifiable factors”, “prevention”, and “calcium”. Boolean operators – AND and OR – were used to refine the search domain. To enhance the efficiency of database querying, the metacharacters .ti and .ab were employed. The metacharacter $ was used to search for plural forms of terms. A total of 67 bibliographic sources were analyzed, with 26 sources retained based on relevance and completeness of information. The languages of the studied bibliographic sources included English, French, Russian, and Romanian.
Primary research. A primary study was planned, which involved the development and validation of a questionnaire for the hygienic estimation of the impact of risk factors on morbidity due to osteoporosis. This study was conducted in five stages: (i) development of the questionnaire, (ii) content validity, (iii) pre-testing, (iv) validity, and (v) internal consistency (Fig. 1).
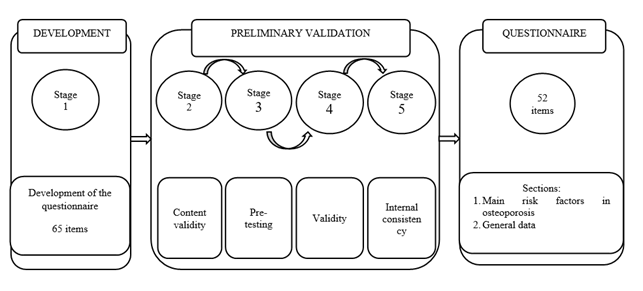 |
Fig. 1 Design of the pre-testing and validation study. |
This study was conducted in accordance with the guidelines established in the Declaration of Helsinki, and all procedures involving participants in the research study were approved by the Research Ethics Committee of the Nicolae Testemițanu State University of Medicine and Pharmacy in the Republic of Moldova, No. 01, dated June 28, 2023. The questionnaire process was conducted face-to-face. Participants were informed about the purpose and outcomes of the study, as well as the potential benefits and risks. Written consent to participate in the study and agreement to answer questions were obtained from each participant.
Stage 1. Development of the questionnaire.
To achieve the research goal, a new working tool was developed titled “Hygienic Estimation of the Impact of Risk Factors on Morbidity Due to Osteoporosis.” The criteria followed for developing the first version of the questionnaire were: (i) Identification of modifiable factors responsible for the development of osteoporosis, including the frequency of drinking water consumption and type of water, the volume and quality of consumed drinking water, knowledge about the mineral composition of drinking water, dietary preferences, alcohol consumption, intake of foods rich in mineral compounds and vitamins, smoking, frequency and intensity of physical activities, and presence of stressful situations; (ii) Identification of specific characteristics in individuals diagnosed with osteoporosis, including knowledge about osteoporosis, diagnosis established and confirmed by a doctor, history of fractures, fracture locations, hereditary history, adherence to prescribed treatment, and data on menopause; (iii) General data: age, biological sex, living environment, body weight, and height. The questionnaire consisted of 3 sections: (i) Modifiable Risk Factors – 44 questions; (ii) Specific Questions for Individuals with Osteoporosis – 14 questions; (iii) General Data – 7 questions. At this stage, the questionnaire included 65 questions.
To minimize measurement errors, the short closed-format questions were designed to be concise and clearly understandable. Additionally, definitions and examples were provided to better clarify the purpose of the questionnaire.
Stage 2. Content validity
This stage involved reviewing the item bank to ensure it measured exactly what was intended. The initial version of the questionnaire was based on the opinions of five medical experts (a rheumatologist, a laboratory physician, a hygiene specialist, a social medicine and management specialist, and a medical imaging specialist) and on a literature search focused on other behavior-based questionnaires and the relationships between risk factors and their impact on the development of osteoporosis. Each expert received a copy of the initial version of the questionnaire via email and was asked to evaluate the tool according to the following criteria: content validity, clarity and comprehensibility, cultural and linguistic relevance, structure and order of questions, and coherence and consistency of the questions. Experts also provided additional comments and suggestions for each item in the questionnaire. As a result, thirteen questions were removed, and eight questions were reformulated, but no new questions were added. At the end of the second stage, the second version of the questionnaire was produced, which included 52 questions, structured as follows: (i) Main Risk Factors in Osteoporosis – 44 questions; (ii) General Data – 6 questions.
Stage 3. Pre-testing
At this stage, both quantitative and qualitative analyses of the questions were conducted to assess their suitability for inclusion in the questionnaire, focusing on validity and internal consistency. A sample of 30 adults from the Republic of Moldova was recruited, who presented themselves at the medical center for the Dual Energy X-ray Absorptiometry (DEXA) investigation, at the doctor's recommendation. Of these participants, 93.3% were female and covered a wide age range. Notably, 21 individuals (70%) had a diagnosis of osteoporosis. The sample was significantly skewed by gender, with an overrepresentation of female participants. The number of subjects included for pre-testing was based on similar studies [8-11]. Data collection occurred from October 2023 to February 2024.
Stage 4. Validity
Participants answered questions from the second version of the questionnaire and a brief ad-hoc questionnaire with three open-ended questions to provide additional feedback on the new questionnaire regarding the ease of understanding and clarity of the questions on fundamental aspects. At this stage, all questionnaires were analyzed based on the degree of completion for each question. All questionnaires met the completion criteria, and none were excluded from the study. For validity, frequencies were calculated, and open-ended responses provided by participants were analyzed to improve the instrument.
Stage 5. Internal consistency
To determine the internal consistency and reliability of the questionnaire, the Cronbach’s Alpha coefficient was calculated based on the linear correlation model. The value of Cronbach’s Alpha ranges between 0 and 1. To be considered consistent, an instrument should achieve a value as close to 1 as possible, with 0.70 generally accepted as a threshold by most researchers. The interpretation of the Cronbach’s Alpha coefficient is provided in Table 1 [12]:
| Table 1. Interpretation of Cronbach’s Alpha coefficient values (Lee J. Cronbach, 1951). | |
Values of the coefficient | Consistency |
Greater than 0.9 | Excellent |
Between 0.7 and 0.9 | Good |
Between 0.6 and 0.7 | Acceptable |
Between 0.5 and 0.6 | Poor |
Less than 0.6 | Unacceptable |
Note: Cronbach's alpha (Cronbach'sα), also known as tau-equivalent reliability or coefficient alpha, is a reliability coefficient and a measure of the internal consistency of tests and measures. It assesses how closely related a group of items is as a whole; a higher value indicates greater reliability. Generally, a Cronbach's alpha of 0.70 or above is considered acceptable, while values above 0.90 may indicate excellent reliability. It was named after the American psychologist Lee Cronbach. | |
Since the questionnaire was designed to identify risk factors for osteoporosis and the questions were not segmented into distinct domains, a consistency analysis of the entire instrument was performed. The reliability test result was 0.768. As a result of this stage, the final version of the questionnaire did not undergo any changes, and no questions were excluded, as all questions were deemed relevant to the research. The Cronbach’s Alpha value indicated an acceptable range of internal reliability for the instrument.
Statistical processing
Statistical processing of the data and determination of the Cronbach’s Alpha coefficient were performed using the licensed IBM SPSS Statistics 27 software. In the statistical analysis, various methods were employed to describe and summarize the data. Descriptive measures such as the mean and standard deviation were calculated to assess central tendency and data dispersion. Additionally, minimum and maximum values, as well as percentages and percentiles, were determined to provide a detailed view of the data distribution. Absolute values were used to illustrate the frequencies or magnitudes of measurements within the analyzed sample.
Results
Development of the questionnaire
The first version of the questionnaire contained 65 questions organized into three sections: (i) Identification of Modifiable Factors Responsible for the Development of Osteoporosis; (ii) Identification of Specific Characteristics in Individuals Diagnosed with Osteoporosis; and (iii) General Data.
The elements of the first section, “Identification of Modifiable Factors Responsible for the Development of Osteoporosis”, included 44 questions: open-ended questions, dichotomous questions, and closed-ended questions with predetermined answers, ranging from 2 to 11 response options. The section “Identification of Specific Characteristics in Individuals Diagnosed with Osteoporosis” included 14 questions: open-ended questions, dichotomous questions, and closed-ended questions with predetermined answers, ranging from 2 to 6 response options. The elements of the “General Data” section included 7 open-ended and closed-ended questions. Respondents had the option to choose multiple answers, but all questions were mandatory.
Content validity
Based on the evaluations and comments from experts, syntactic and semantic reformulations and modifications were made to the three sections of the questionnaire, including the removal of 13 irrelevant or repetitive questions. Specifically, 11 questions were removed from the section “Identification of Modifiable Factors Responsible for the Development of Osteoporosis,” one question was removed from the section “Identification of Specific Characteristics in Individuals Diagnosed with Osteoporosis,” and one question was removed from the section “General Data.” As a result, the second version of the questionnaire had a total of 52 questions, restructured into two sections: (i) Major Risk Factors for Osteoporosis and (ii) General Data.
Pre-testing and validity
At the pre-testing stage, according to the respondents’ opinions, the order and content of the questions were found to be good. In face-to-face questioning, all respondents (100%) stated that the questions were clear and easy to understand. However, in 4 (7.7%) questions, respondents suggested replacing some specialized terms with synonyms. As a result, minimal changes were made, specifically related to the terms used to denote certain symptoms. These terms were corrected before the final administration of the questionnaire. The average time for face-to-face questioning was 14.19 minutes. The time range, from a minimum of 11.90 minutes to a maximum of 17.33 minutes, suggests that there is relatively little variation in the duration of the interviews, all falling within a margin of approximately 5.43 ± 1.567 minutes (M ± SD), indicating that most of the interview durations are relatively close to the average of 14.19 minutes.
The questionnaire was revised several times regarding syntax and semantics to avoid ambiguity and errors, after considering the respondents’ reviewed results, pre-testing comments, and experts’ suggestions and opinions. These measures were taken to ensure that the questions in the final questionnaire could competently evaluate each subject and address the study’s objectives.
Characteristics of the sample
The socio-demographic characteristics of the individuals who participated in the pre-testing phase of the questionnaire are presented in Table 2 and Table 3.
Table 2. The demographic and anthropometric characteristics of the respondents: pre-testing stage. | ||||
| Mean | ± SD | Min | Max |
Age, years | 50.37 | 2.6 | 25 | 72 |
Body weight, kg | 70.75 | 2.03 | 43.5 | 94.0 |
Height, cm | 165.03 | 1.25 | 152.0 | 182.0 |
Note: SD - Standard Deviation; Min – minimum; Max – maximum; kg – kilograms; cm – centimeters. | ||||
The respondents’ ages ranged from 25 to 72 years, with a mean age of 50.37 ± 2.6 years. The average body weight of the participants was 70.75 kg, with a standard deviation of ± 2.03 kg, indicating moderate variation in body weight among individuals. The lowest recorded weight was 43.5 kg, and the highest was 94.0 kg. This variability may reflect different levels of physical activity, types of body constitution, and possibly different dietary habits among participants. The average height of the participants was 165.03 cm, with a standard deviation of ± 1.25 cm. The minimum recorded height was 152.0 cm, and the maximum was 182.0 cm.
Table 3. Demographic and educational profile of respondents: pre-testing stage. | ||
| No | % |
Gender | ||
| 2 | 6.7 |
| 28 | 93.3 |
Total Gender | 30 | 100 |
Living Environment | ||
| 16 | 53.3 |
| 14 | 46.7 |
Total Living Environment | 30 | 100 |
Education | ||
| 5 | 16.7 |
| 8 | 26.7 |
| 17 | 56.6 |
Total Education | 30 | 100 |
Note: No - the absolute number; % - percent | ||
As shown in Table 3, the gender distribution of a sample of 30 respondents was analyzed. Of these, 28 (93.3%) were female and 2 (6.7%) were male. To better understand the data distribution, the median, 25th percentile (Pr25), and 75th percentile (Pr75) were calculated. The gender distribution analysis indicates a clear predominance of the female gender. Most central and dispersion values (median, Pr25, and Pr75) are “Female,” reflecting the imbalanced gender distribution in this sample. It is noteworthy that respondents were similarly sampled from both urban (53.3%) and rural (46.7%) environments. Most respondents (56.6%) reported having higher education, followed by those with secondary vocational education (26.7%) and those with no education (16.7%).
Internal consistency
Out of the 52 questions subjected to the consistency analysis, 5 open-ended questions and 6 questions from the “General Data” section, which could not be coded, were excluded. The Cronbach’s Alpha coefficient was 0.768, demonstrating good consistency.
Table 4. Statistical analysis of questionnaire items. | |||||
| Mean Scale if Item is Excluded | Scale Variance if Item is Excluded | Corrected Item-Total Correlation | Cronbach’s Alpha if Item is Excluded | Decision |
Q1 | 106.43 | 116.286 | 0.575 | 0.757 |
|
Q2 | 106.57 | 121.619 | 0.097 | 0.767 |
|
Q3 | 106.71 | 122.571 | 0.000 | 0.768 |
|
Q4 | 106.71 | 122.571 | 0.000 | 0.768 |
|
Q5 | 106.57 | 121.619 | 0.097 | 0.767 |
|
Q6 | 106.57 | 121.619 | 0.097 | 0.767 |
|
Q7 | 106.43 | 116.286 | 0.575 | 0.757 |
|
Q8 | 106.57 | 123.619 | -0.142 | 0.771 | Item retained |
Q9 | 106.71 | 122.571 | 0.000 | 0.768 |
|
Q10 | 106.57 | 123.619 | -0.142 | 0.771 | Item retained |
Q11 | 106.71 | 122.571 | 0.000 | 0.768 |
|
Q12 | 106.71 | 122.571 | 0.000 | 0.768 |
|
Q13 | 106.43 | 119.286 | 0.286 | 0.763 |
|
Q14 | 106.43 | 121.619 | 0.066 | 0.768 |
|
Q15 | 105.57 | 123.619 | -0.092 | 0.780 | Item retained |
Q16 | 105.57 | 104.286 | 0.677 | 0.739 |
|
Q17 | 105.71 | 116.571 | 0.111 | 0.776 | Item retained |
Q18 | 106.57 | 115.286 | 0.880 | 0.754 |
|
Q19 | 103.43 | 115.619 | 0.393 | 0.758 |
|
Q20 | 103.14 | 116.143 | 0.533 | 0.757 |
|
Q21 | 103.57 | 114.619 | 0.506 | 0.755 |
|
Q22 | 106.00 | 118.000 | 0.409 | 0.761 |
|
Q23 | 106.14 | 115.143 | 0.623 | 0.755 |
|
Q24 | 106.43 | 116.286 | 0.575 | 0.757 |
|
Q25 | 106.43 | 121.619 | 0.066 | 0.768 |
|
Q26 | 106.71 | 122.571 | 0.000 | 0.768 |
|
Q27 | 106.00 | 118.000 | 0.409 | 0.761 |
|
Q28 | 106.00 | 117.333 | 0.285 | 0.762 |
|
Q29 | 106.29 | 108.238 | 0.838 | 0.741 |
|
Q30 | 106.00 | 119.000 | 0.313 | 0.763 |
|
Q31 | 105.57 | 106.619 | 0.577 | 0.745 |
|
Q32 | 105.57 | 118.286 | 0.135 | 0.769 | Item retained |
Q33 | 106.71 | 122.571 | 0.000 | 0.768 |
|
Q34 | 106.00 | 117.333 | 0.285 | 0.762 |
|
Q35 | 106.57 | 115.286 | 0.880 | 0.754 |
|
Q36 | 106.00 | 122.000 | 0.031 | 0.769 | Item retained |
Q37 | 106.71 | 122.571 | 0.000 | 0.768 |
|
Q38 | 106.71 | 122.571 | 0.000 | 0.768 |
|
Q39 | 105.57 | 121.619 | 0.097 | 0.767 |
|
Q40 | 105.71 | 117.905 | 0.226 | 0.764 |
|
Q41 | 106.43 | 115.286 | 0.673 | 0.755 |
|
Note: Q - question | |||||
It should be noted that excluding certain questions may increase the Cronbach’s Alpha coefficient (Table 4). If questions Q8 and Q10 are excluded, the coefficient could potentially rise to 0.771. For question Q15, it could increase to 0.780; if question Q17 is excluded, it could rise to 0.776; and if questions Q32 and Q36 are excluded, it could be 0.769. Given that these questions are relevant to the research and will provide unique and qualitative information, the decision was made to retain them in the current version of the questionnaire without any modifications.
Discussions
This study aimed to develop and test a new questionnaire designed for the hygienic assessment of the impact of risk factors, particularly modifiable ones, on morbidity due to osteoporosis. Our results indicate that the new instrument was considered by experts to have good clarity and relevance. Respondents found the questionnaire acceptable and easy to understand, demonstrating its validity. Additionally, the Cronbach’s Alpha coefficient was 0.768, which further confirms that the responses across the questions are well correlated.
In the context of recent literature [13, 14], new questionnaires have been developed and validated to assess people's knowledge and perceptions about osteoporosis. Generally, these questionnaires have focused on studying knowledge, attitudes, and practices regarding osteoporosis from various perspectives [15-20]. However, few studies focus on developing questionnaires aimed at highlighting modifiable risk factors, such as the mineral composition of drinking water. Most frequently, studies provide information about both modifiable and non-modifiable risk factors for osteoporosis, contributing to its development. They also highlight common risk factors such as age, sex, family history, dietary habits, physical activity level, smoking, and alcohol consumption [20].
In the study that evaluated the knowledge, attitudes, and practices of adult patients at Bashair Hospital, Sudan, regarding osteoporosis [21], it was revealed that factors such as age, education level, and sex had a notable influence on the levels of knowledge and practices concerning some modifiable risk factors responsible for the development of osteoporosis. Our results are consistent with these findings, highlighting the acceptability and clarity of the questionnaire among respondents from various living environments and education levels.
Another study conducted by Barik S. et al. (2022) focused on the translation and adaptation of the OKAT (Osteoporosis Knowledge Assessment Tool), which consisted of 20 questions designed to assess knowledge about osteoporosis, risk factors, prevention, and treatment options. The Cronbach’s Alpha coefficient was calculated to measure internal consistency, obtaining a value of 0.892. The results showed good readability and consistency of the OKAT instrument. The average score obtained by participants was 11.3 ± 2.1, indicating a low level of knowledge about osteoporosis. Significant differences in scores were observed based on education level and family history of osteoporosis or fractures [22]. In comparison, the Cronbach’s Alpha coefficient of 0.768 indicates good internal consistency, suggesting that our questionnaire is a reliable tool for measuring modifiable risk factors.
These findings highlight the importance of developing reliable and valid assessment tools for measuring knowledge and practices related to osteoporosis, considering modifiable risk factors. The implementation of such questionnaires can help improve educational programs and preventive strategies, thereby contributing to the reduction of morbidity due to osteoporosis [23].
The development of the questionnaire included several stages, such as pre-testing and content validation, which led to the elimination and reformulation of some questions to improve their clarity and relevance. The socio-demographic characteristics of the individuals who participated in the pre-testing phase showed a diversity of age, gender, and living environment, contributing to the overall validity of the instrument.
These findings are consistent with those reported in specialized literature. Previous studies have emphasized the importance of developing reliable and valid assessment tools for measuring knowledge and practices related to osteoporosis. Moreover, research has shown that modifiable risk factors, such as diet and physical activity, play a significant role in the prevention of osteoporosis [24-26]. Our study results support these conclusions and suggest that the new questionnaire can be an effective tool for evaluating and improving osteoporosis prevention strategies.
Conclusions
The study demonstrated that the new questionnaire is a valid and reliable tool for assessing the impact of modifiable risk factors on morbidity due to osteoporosis. It can be used in various contexts to enhance preventive knowledge and practices, thereby contributing to a reduction in osteoporosis incidence. Further research is needed to refine and validate this questionnaire in broader populations to ensure its applicability and utility on a larger scale.
Competing interests
None declared.
Authors’ contributions
All the authors participated in the study design and contributed to drafting the manuscript. The authors critically reviewed the work and approved the final version of the manuscript.
Acknowledgment
No external funding.
Patient consent
Obtained.
Ethics approval
The study was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy in the Republic of Moldova, Minutes No.01, dated June 28, 2023.
Limitations
A significant limitation of this study is the inability to establish criterion validity, defined as the degree of agreement between the new questionnaire and another measure of the construct that serves as a benchmark or gold standard. This limitation arises because no standardized analogous questionnaire was identified in the specialized literature. Most available questionnaires in the field are of the KAP (Knowledge, Attitudes, and Practices) type, which prevented the use of a recognized benchmark for criterion validation of the new questionnaire. In this research, the pilot testing phase of the questionnaire was not conducted because the overall sample size calculated for the main study was 296 individuals diagnosed with osteoporosis. Recruiting the required number of individuals with osteoporosis proved challenging due to time constraints and additional costs.
Authors’ ORCID IDs
Victoria Bologan – https://orcid.org/0009-0009-2518-3847
Lucia Mazur-Nicorici – https://orcid.org/0000-0003-3983-8292
Larisa Spinei – https://orcid.org/0000-0002-5370-9801
Serghei Cebanu – https://orcid.org/0000-0002-2493-4882
Anatolie Visnevschi – https://orcid.org/0000-0001-9664-7527
Elena Ciobanu – https://orcid.org/0000-0002-8969-922X
References
World Health Organization (WHO). Simple ways to prevent osteoporosis [Internet]. Geneva: WHO; 2019 [cited 2024 July 25]. Available from: https://www.who.int/westernpacific/articles/item/simple-ways-to-prevent…
Kanis JA, McCloskey EV, Johansson H, Cooper C, Rizzoli R, Reginster JY. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int. 2013;24(1):23-57. doi: 10.1007/s00198-012-2074-y.
Black DM, Rosen CJ. Clinical practice. Postmenopausal osteoporosis. N Engl J Med. 2016;374(3):254-262. doi: 10.1056/NEJMcp1513724.
Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures. Lancet. 2002;359(9319):1761-1767. doi: 10.1016/S0140-6736(02)08657-9.
Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17(12):1726-1733. doi: 10.1007/s00198-006-0172-4.
Nguyen ND, Frost SA, Center JR, Eisman JA, Nguyen TV. Development of prognostic nomograms for individualizing 5-year and 10-year fracture risks. Osteoporos Int. 2008;19(10):1431-1444. doi: 10.1007/s00198-008-0588-0.
Gendler PE, Coviak CP, Martin JT, et al. Revision of the Osteoporosis Knowledge Test: reliability and validity. West J Nurs Res. 2015;37(12):1623-1643. doi: 10.1177/0193945914537565.
Dawson B, Trapp RG. Basic & Clinical Biostatistics. 4th ed. New York: McGraw Hill Professional; 2004. 416 p.
Goni L, Gil M, de la O V, Martínez-González MÁ, Eisenberg DM, Pueyo-Garrigues M, Vasilj M, Gayoso L, Etxeberria U, Ruiz-Canela M. Development and validation of a new home cooking frequency questionnaire: a pilot study. Nutrients. 2022;14(6):1136. doi: 10.3390/nu14061136.
AbuQamar M, Tabash MI, Aish A, Hasheesh AA, Sharaf F. Health impact of drinking water quality on the occurrence of osteoporosis in Gaza Strip, Palestine. Ethiop J Health Sci. 2023;33(5):841-850. doi: 10.4314/ejhs.v33i5.14.
Yong TSM, Panting AJ, Juatan N, et al. Development and validation of a cognitive, affective and behaviour questionnaire on pet-associated zoonotic diseases (CAB-ZDQ). Vet Med Sci. 2021;7(5):1558-1563. doi: 10.1002/vms3.547.
Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16(3):297-334. https://doi.org/10.1007/BF02310555.
Croitoru C, Ciobanu E, Ferdohleb A. Validarea chestionarului: Cunoștințe, Atitudini și Practici privind fenomenul de antibiorezistență la medici [Validation of questionnaire: Knowledge, Attitudes and Practices regarding the antibioresistance phenomenon to doctors]. Arta Medica. 2022;84(3):4-15. Romanian. doi: 10.5281/zenodo.7305448.
Ferdohleb A, Croitoru C, Ciobanu E, Tapu L, Spinei L. Questionnaire standardization knowledge, attitudes, and practices regarding the antimicrobial resistance of medical workers. In: Biomedical and health research: quality, excellence and performance, 19-21 October 2022, Chișinău, Republic of Moldova: Abstract book. Chișinău; 2022. p. 67.
Ahmed S, Farooqui AJ, Pradhan NA, et al. Assessing the knowledge, attitude and practice of osteoporosis among Pakistani women: a national social-media based survey. PLoS One. 2023;18(11):e0288057. doi: 10.1371/journal.pone.0288057.
Gaines JM, Marx KA, Narrett M, Caudill J, Landsman J, Parrish JM. Validation of the male osteoporosis knowledge quiz. Am J Mens Health. 2011;5(1):78-83. doi: 10.1177/1557988310363816.
Mahdaviazad H, Keshtkar V, Emami MJ. Osteoporosis guideline awareness among Iranian family physicians: results of a knowledge, attitudes, and practices survey. Prim Health Care Res Dev. 2018;19(5):485-491. doi: 10.1017/S1463423618000014.
Eslami-Mahmoodabadi A, Foroughameri G, Maazallahi M, Farokhzadian J. Nurses’ knowledge, attitude, and practice regarding osteoporosis prevention and its correlation with their nutritional behaviors. J Prev Med Hyg. 2024;64(4):E429-E437. doi: 10.15167/2421-4248/jpmh2023.64.4.2709.
Nohra J, Sacre Y, Abdel-Nour A, Mannan H. Evaluation of knowledge, attitudes, and practices related to osteoporosis and correlates of perceived high risk among people living in two main districts of Lebanon. J Osteoporos. 2022;2022:1188482. doi: 10.1155/2022/1188482.
Alani Q, Yassir M, Mansoor R, et al. Knowledge, attitude, and practices towards osteoporosis among adults in the United Arab Emirates (UAE) in 2023. Cureus. 2024;16(3):e56084. doi: 10.7759/cureus.56084.
Abdo HAA, Idris SM. Knowledge, attitude and practice of osteoporosis among adult patients in Bashair hospital, Sudan, 2021. EAS J Psychol Behav Sci. 2022;4:83-91. doi: 10.36349/easjpbs.2022.v04i03.001.
Barik S, Raj V, Munshi B.D, Rajput O, Prajapati S, Prasad S.G, Kumar A. Development and validation of India-specific Hindi version of osteoporosis knowledge assessment tool. J Mid-life Health. 2023;14(4):252-256. doi: 10.4103/jmh.jmh_219_22.
Zhang Q, Cai W, Wang G, Shen X. Prevalence and contributing factors of osteoporosis in the elderly over 70 years old: an epidemiological study of several community health centers in Shanghai. Ann Palliat Med. 2020;9(2):231-238. doi: 10.21037/apm.2020.02.09.
Taghvaei R, Dimitrova D, Karaman M, et al. Knowledge and understanding risk factors and preventive measures for osteoporosis in women: results of a survey in 502 women with and without a migration background. BMC Musculoskelet Disord. 2022;23:824. doi: 10.1186/s12891-022-05773-0.
von Hurst PR, Wham CA. Attitudes and knowledge about osteoporosis risk prevention: a survey of New Zealand women. Public Health Nutr. 2007;10(7):747-753. doi: 10.1017/S1368980007441477.
Oh SM, Song BM, Nam BH, et al. Development and validation of osteoporosis risk-assessment model for Korean men. Yonsei Med J. 2016;57(1):187-196. doi: 10.3349/ymj.2016.57.1.187.