
Introduction
Chronic hepatitis Delta virus (HDV) -induced liver disease continues to be a major cause of premature mortality despite impressive advances in the prevention of chronic viral infections [1].
HDV prevalence is globally descending, a phenomenon explained by the introduction of primary prophylaxis with the approval of HBV vaccination programs. But despite this, endemic areas are still registered. Republic of Moldova is a region of „endemic pocket” for HDV, according to the latest international statistics [1-3]. The course of this infection is dependent on the condition of infection with HBV (coinfection or superinfection), as well as a multitude of viral and host factors such as age, gender, immune status, HBV genotype and/or HDV genotype, HBeAg status that will direct the disease to possible moderate or even fulminant progression or induce chronic liver process. The peculiarities of chronic liver disease attributed to HDV in the evolutionary-progressive framework, note multiple fatal complications in the younger age of the patient [4-6].
According to the National Liver Transplant Registry, about 70% of patients on the waiting list have terminal HDV-induced liver disease [7]. Although it is associated with high mortality, the decompensation of HDV-induced liver disease is one of the preventable causes of death worldwide [1, 5]. The main objective of this study is to estimate the DALY of HDV liver disease and make a comprehensive quantification of the burden of the disease in terms of years lived with disability. It can be used effectively to educate people about the year lost due to the premature death of a patient who develops HDV-induced cirrhosis and the time these patients lose from disability cause. This step can allow policy makers to understand the severity of the problem more explicitly and encourage more effective public spending on health and disease prevention [8].
We mention that the course of infection with the delta hepatitis virus also depends on the condition of infection, according to which we may have coinfection between HBV and HDV and superinfection between HDV and chronic HBV infection. Coinfection between these two viruses more commonly develops forms of severe or fulminant hepatitis than acute viral infection B. On the other hand, acute infection with HDV is imperceptible to an ordinary infection with HBV, from a clinical and histological point of view [2, 3, 5]. Thus, the clinical course of chronic HDV infection is still dependent on the course of liver disease induced by chronic B viral infection. Chronic viral hepatitis Delta is more severe and rapid-progressive versus other chronic viral hepatitis known. This leads to cirrhosis in about 70% of patients within 5 to 10 years, usually involving the young working class. The risk of developing cirrhosis is 3 times higher in case of a HDV infection than in case of a mono-HBV infection [5, 9-11].
Material and methods
For the social impact assessment based on the DALY indicator, 104 patients (46 men and 58 women) with HDV-induced liver disease, mean age of 56±4.5 years, were selected. Demographic distribution of patients Central area – 54%, South area – 36%, North area – 10%. There were also analyzed aspects of the natural evolution of the disease with the progression to cirrhosis of the liver, taking into account further and installed complications that can affect the quality of life, such as ascites, hepatic encephalopathy, variceal bleeding, development of hepatocellular carcinoma (HCC) or death. This is an analytical prognostic study. The representative research batch was calculated in the F tests Program - ANOVA: Fixed effects, omnibus, one-way Analysis: Calculations are based on the following parameters: the confidence interval for 95.0% of significance of the results, statistical power – of 80.0%. Result: noncentality parameter = 9.9375000, critical F = 3.0540042, numerator df = 2, denominator df = 175, total for research = 194. The given study is part of the research protocol that obtained a favorable opinion from the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (No.5 dated 17.06.2022). The study is still continuing. The patients enrolled in the study were hospitalized in the Hepatology Department of a tertiary Centre and Therapy section of the Medical Service of Municipal Centre Chisinau for 2021-2024 years interval. Data on the onset of the disease, duration until liver cirrhosis, progression in months/years until the registration of complications or death were collected from the discussion with patients, by collecting anamnestic data, analysis of the medical archive, and the medical record of the patient from the stationary 003/e form.
Clinical informatics data were being analyzed in Microsoft Excell and SPSS statistical analysis software. Several data processing steps were undertaken.
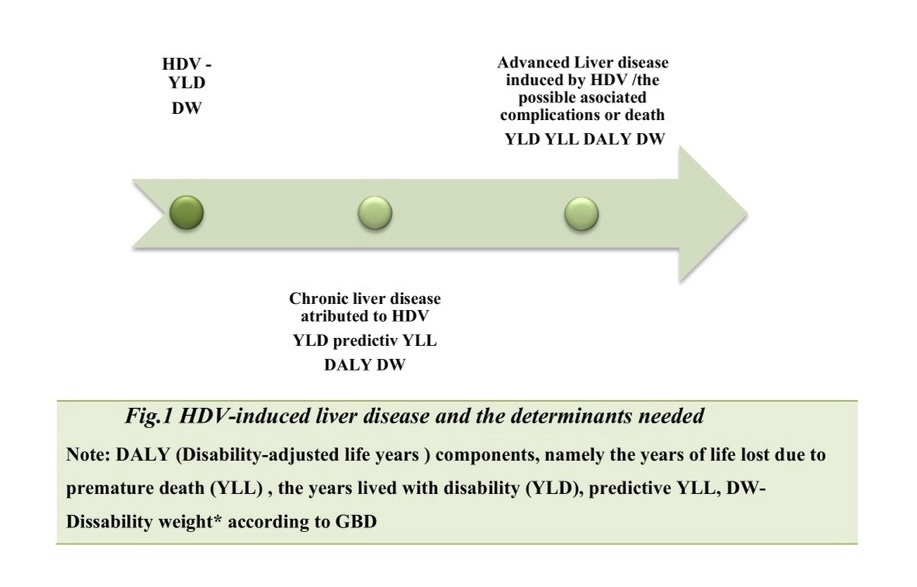
Qualitative representation of the progression of the disease by ordering all relevant health results related to the disease over time, with reflection of the intense dynamic effect of the disease were taken into account. The DALY components, namely the years of life lost due to premature death (YLL) and the years lived with disability (YLD), were calculated separately for all health outcomes included in the final tree, initially stratifying the impact in patients with moderate liver disease then the impact on progression to advanced liver disease, then the association of complications or death. Thus, we aim to mark the scale of disease progression and its impact in years of life, at each stage of the disease (Fig.1).
Next, we are going to analyze the social impact produced by HDV-induced liver disease through the following methodology: initially, the WHO-proposed indicator for this purpose is YLD – years lived with disability or altered behavior and/or motor faculties. In order to estimate YLD for a particular disease over a certain period of time, the number of cases in this period is multiplied by the average duration of the disease and the impact coefficient of disability, and, reflecting the severity of the disease on a scale from 0 (perfect health) to 1 (death). The disability impact coefficient is found in the Global Burden of Disease (GBD) source [12-14]. The basic formula without applying the social aspects for calculating YLD includes the following
YLD = I x L x DW
In this formula I – number of incident cases in the population, DW – disability weight of specific condition, and L – average duration of the case until remission or death (years).
How much a medical condition affects a person is called the disability weight (DW). This is determined by disease or disability and does not vary with age. Tables have been created for thousands of diseases and disabilities. In the GBD terminology, the term disability is used broadly to refer to departures from optimal health in any of the important domains of health in GBD. According to research analysis of the Global Burden of Disease 2019 Study, leading causes of global DALYs, percentage of total DALYs, and percentage change in number of DALYs and age-standardized DALY rates from 1990 to 2019 for both sexes combined for all ages, cirrhosis of the liver ranks as 16th leading causes of disability-adjusted life years, in the < 49 age group being the 12th cause. Cirrhosis ranked seventh among those aged 50-74 years in 2019. With low-cost treatments available to low-income and middle-income countries, there is an opportunity to eradicate hepatitis C, but still remains a problem regarding HDV. Childhood vaccinations for hepatitis B will eventually also reduce cirrhosis (and HCC) outcomes, but the full effect will probably not be apparent for years. Its contribution to the global disease burden has increased from 24.3 million in 1990 to more than 31 million in 2019, which represents a 27% increase in DALYs. But while health has improved, after accounting for population growth and ageing, the absolute number of DALYs has remained stable [14].
Results
Referring to our study compared to the average duration of a case of disease in a patient with Delta viral hepatitis in males – 18.86, is recorded a total YLD of 127.86, and in the case of liver cirrhosis at an average duration of a disease case of only 6.20, there is a total YLD of 619.34 and a media of 14.90 (95% Cl: 3.95-33.77 ), this means that advanced liver disease shows a substantially impact on patients. Table 1 provides an average age of onset of advanced liver disease in men 45.35, and 45.87 women with an average duration of one case from its onset to enrolment in the study of 6.2 in the male gender and 6.56 in women. The highest value of YLD is recorded in the group of men within age category of 60-74 years being 23.43 YLD, while in women a higher YLD number remarks in 30-44 category with a value of 20.69 YLD
Table 1. Years lived with disability due to HDV-induced liver disease by gender-dependent age groups (in YLD) | |||||||
No. | Age group | Patients gender | Nr. Of cases | Mean age of the onset of the disease | Average duration of the case | DW | Years lived with disability YLD |
1 | 30-44 (16) | M | 10 | 33.4 | 5.2 | 0.716 | 124.35/12.43 |
F | 6 | 34.67 | 5.0 | 0.716 | 124.11/20.69 | ||
2 | 44-59 (45) | M | 24 | 45.17 | 6.58 | 0.716 | 212.80/8.86 |
F | 21 | 46.71 | 6.71 | 0.716 | 312.70/14.89 | ||
3 | 60-74 (43) | M | 12 | 57.5 | 6.83 | 0.716 | 282.19/23.43 |
F | 31 | 56.25 | 7.97 | 0.716 | 320.99/10.35 | ||
Total/Average | M | 46 | 45.35 | 6.20 | - | 619.34/14.90 | |
F | 58 | 45.87 | 6.56 | - | 757.80/15.31 | ||
Note: YLD - Years lived with disability due to HDV-induced liver disease, DW - Disability weight according to GBD [2,14] | |||||||
Compared to the average duration of a male patient's disease case at an average duration of a disease case of only 6.20, there is a YLD total of 619.34 and a per person media of 14.90 (95% Cl: 3.95-33.77 ) , this explains the severity of the disease, with substantial social impact. Thus, among female patients at an average duration of a case of 6.56 with a total YLD of 757.80 and an individual media of (95% Cl
: 2.43-28.18) . When the disease progresses to mortality 17 patients had an YLD with a value of 1668.7 in men and 1102.67 in women.
As a component in math formula for DALY specifically important is YLL – the life years lost as a result of premature deaths practically correspond to the number of deaths caused by a disease multiplied by the indicator of life expectancy at the age at which death occurs. The basic formula for YLL (not including other social aspects) is the following for a particular disease, age and gender; includes the following: YLL = N x L where: N – number of deaths, L – life expectancy at the age of death in years [8].
Although the YLL measure was proposed in the 1940s, the creation of the GBD and its associated methodological developments have increased awareness and understanding of its application, although many issues are still being challenging. First, it is important to articulate that the 'true' YLL can never be observed and as such, a language indicating that YLL estimates have been under-estimated or over-estimated or maybe pseudo-interpreted. From the perspective of public health policy information, the element to be applied in the YLL estimate is that of an ideal, aspirational standard based on low mortality risks [15]. Premature mortality refers to the anticipated death for the age at which the person could have survived if they were part of a model-standardized population with a life expectancy equal to that of a maximum long-term population in the given region, information reflected individually by each country, specific data of the Republic of Moldova is generated by the National Bureau of Statistics last edition 2022 [13-15]. To estimate population health loss due to advanced liver disease is a largely contested fact. This has led to the application of different approaches for estimating lost life years due to premature mortality (YLL). The YLL was predicted by using the Child-Pugh estimate of the remaining years of life. Based on recent laboratory reports of bilirubin, albumin, prothrombin time (INR), and clinical assessment of ascites and encephalopathy, the Child-Pugh Score calculator identifies patients in one of three risk classes: class A (5 to 6 points): Life expectancy is 15-20 years, class B (7 to 9 points): Life expectancy is 4-14 years, class C (10 to 15 points): Life expectancy 1-3 years.
The Child-Pugh score was used to estimate the remaining life years and this number was subtracted from the ideal age-specific life expectancy to allow us to calculate YLL not just for the 16.34% of patients from the total group, this data reflecting the mortality rate.
The index of YLL due to early mortality first was calculated for the 17 deceased patients, the mean age of onset of liver cirrhosis was 45.84 years with mean disease duration of about 16.95 years. Preterm mortality associated with advanced liver disease induced by HDV with the highest incidence was attested in the 30-44-year age group (Table 2). Of the total age groups, 45–59-year-olds had the highest YLL index for both women and men with a total of 164 YLL. For women, the highest rate of major premature mortality associated with advanced HDV-induced liver disease is recorded in the 44-59-year group – 79.2 YLL. The data for 30-44-year group, men lost 94.2 YLL. The data presented reveal that premature mortality associated with advanced HDV-induced liver disease and the fact that the disease occurs more frequently in the 45–59-year age group, the lowest values of YLL were in the 60–74-year-old group where the YLL number was 46.0 for men and 56.4 for women. Overall, men lost 225.6 years as a result of premature mortality, and women – 135.6 years. By the age of about 59 the proportion of YLL increases, after which a slight decrease is subsequently perceived (Table 2). Moreover, we are seeing an increase in the burden of male mortality, which may indicate the fact of a later addressability. This situation underlines the need for effective prevention policies aimed at men's health.
Table 2. Life years lost as a result of premature mortality associated with advanced liver disease induced by HDV by gender-dependent age groups, for deceased patients (in YLL) | ||||||
No. | Age group | Gender | N. of cases | Mean age of death | Life expectancy at the age of death in years* | YLL |
1 | 30-44 | M | 3 | 38.66 | 31.6 | 94.8 |
F | 0 | 0 | 0 | 0 | ||
2 | 45-59 | M | 4 | 51.25 | 21.2 | 84.8 |
F | 3 | 52.57 | 26.4 | 79.2 | ||
3 | 60-74 | M | 4 | 66.5 | 11.5 | 46.0 |
F | 3 | 61.33 | 18.8 | 56.4 | ||
Total/Mean | M | 11 | 52.11 | 20.4 | 225.6/20.5 | |
F | 6 | 56.95 | 23.0 | 135.6/22.6 | ||
Note: YLL - Life years lost as a result of premature mortality *according to the data of the National Bureau of Statistics of the Republic of Moldova 2022 [16] | ||||||
Thus, with all the above mentioned, we set out to calculate the DALY index, by predictive YLL, in living patients according to the severity of the disease by means of Child Pugh classification, this phenomenon being also applied in other studies. So we were able to establish a predictive YLL in 46 males with a total of 246.36 YLL in a mean age of death 58.34 and in 58 women a value of 239.83 predictive YLL in a mean age of death 64.55 (Table 3).
Table 3. Life years lost as a result of premature mortality associated with advanced liver disease induced by HDV by gender-dependent age groups, (in predictive YLL) | ||||||
No. | Age group | Gender | N. of cases | Mean age of death | Life expectancy at the age of death in years* | Predictive YLL |
1 | 30-44 (16) | M | 10 | 45.30 | 25.7 | 250.70 |
F | 6 | 48.50 | 30.0 | 180.00 | ||
2 | 45-59 (45) | M | 24 | 59.41 | 15.6 | 374.40 |
F | 21 | 69.71 | 12.7 | 266.70 | ||
3 | 60-74 (43) | M | 12 | 70.33 | 9.5 | 114.00 |
F | 31 | 75.45 | 8.8 | 272.80 | ||
Total/Mean | M | 46 | 58.34 | 16.93 | 246.36/5.35 | |
F | 58 | 64.55 | 17.16 | 239.83/4.13 | ||
Note: Predictive YLL-predictive life years lost as a result of premature mortality, *according to the data of the National Bureau of Statistics of the Republic of Moldova 2022 [16] | ||||||
Here in the context of the disease state with evolution in death we allow ourselves to calculate DALY the indicator proposed by WHO for this purpose – (Disability Adjusted Life Years). DALYs are calculated by taking the sum of these two components: DALY = YLD + YLL.
The DALY relies on an acceptance that the most appropriate measure of the effects of chronic illness is time. One DALY, therefore, is equal to one year of healthy life lost [14].
Table 4. DALY associated with advanced liver disease induced by HVD by age groups dependent on person-gender | |||||||
No. | Age group | Gender | N. of cases | YLD | Predictive YLL | DALY | |
Total | Per person | ||||||
1 | 30-44 | M | 10 | 124.35 | 250.70 | 375.05 | 37.50 |
F | 6 | 124.11 | 180.00 | 304.11 | 50.68 | ||
2 | 45-59 | M | 24 | 212.80 | 374.40 | 587.20 | 24.47 |
F | 21 | 312.70 | 266.70 | 579.40 | 27.59 | ||
3 | 60-74 | M | 12 | 282.19 | 114.00 | 396.19 | 33.01 |
F | 31 | 320.99 | 272.80 | 593.79 | 19.15 | ||
Total by groups | M | 46 | 619.34 | 739.10 | 1358.44 | 29.53 | |
F | 58 | 757.80 | 719.50 | 1477.30 | 25.47 | ||
Media by groups | M | 206.44 | 246.36 | 452.81 (95% Cl: 162.51-743.11) | |||
F | 252.60 | 239.83 | 492.43 (95% Cl: 86.89-897.97) | ||||
Note: YLD - Years lived with disability, predictive YLL- Life years lost as a result of premature mortality predictive, DALY Disability Adjusted Life Years | |||||||
Based on the above data, the value of the DALY indicator lost by the three groups according to age can be determined (Table 4).
Thus, it was established that male patients aged 30-44 years lost 375.05 DALYs and per person 37.5 DALY. Men aged 45-59 years lost 587.2 DALYs per person – 24.47 DALY; in the age group of 45-59 years female gender losses were: 579.4 DALY. At the age group of 60-74 years it was determined that the men lost – 396.19 DALYs, per person – 33.01 DALY; and in women of this age – 593.79 DALYs and 19.15 per person. With a total of 1358.44 DALY men, that is, in the environment each of them losing about 29.53 DALY as a result of disability during the period they were sick and because of premature death caused by the disease. While the 58 women lost 1477.3 DALYs or an average of 25.47 per person. The media per groups reflected in table indicate 452.81 (95% Cl: 162.51-743.11) in males , and 492.43 (95% Cl: 86.89-897.97) in females. We attest a DALY value per person higher in the group of young people, people able to work.
17.64% of the total number of enrolled patients developed HCC, with installation at an average age of 61 years, of which 35.29% resulted in death within the first 3 months of diagnosis. In males a media value of 20.24 (95% Cl: 14.59-25.89) YLL , in females 18.28 (95% Cl: 14.13-22.44) YLL. While the value of YLD With the advancement of the hepatic process, with progression towards the onset of complications such as the presence of liver cancer, the study attests a DALY value per person increasing – DALY per person in males being 32.01 and females 39.69 (Table 5) compared to patients without any, DALY per person male 31.66 and female-32.47 (Table 4).
Table 5. DALY indicator in HCC on the background of HDV-induced liver cirrhosis by gender-dependent age group (in YLD) | |||||||||
No. | Age group | Gender | Onset medium age | Average duration of a case | DW** | YLD | YLL | DALY | DALY |
Total | Per pers | ||||||||
1 | 44-59 | M (6) | 28.50 | 19.66 | 0.857 | 101.09 | 144.8 | 245.89 | 40.98 |
F (2) | 46.00 | 7.00 | 0.857 | 11.99 | 51.20 | 63.19 | 31.59 | ||
2 | 60-74 | M (3) | 51.33 | 12.33 | 0.857 | 31.70 | 37.4 | 69.1 | 23.03 |
F (6) | 24.42 | 37.28 | 0.857 | 191.69 | 95.1 | 286.79 | 47.79 | ||
Total/Media | M (9) | 39.91 | 28.47 | - | 132.79 14.75 | 182.2/l 20.24 | 314.99 | 32.01 | |
F (8) | 35.21 | 22.14 | - | 203.68 25.46 | 146.3/ 18.28 | 349.98 | 39.69 | ||
Note: YLD - Years lived with disability, YLL- Life years lost as a result of premature mortality, DALY- Disability Adjusted Life Years **according to the data of Global Burden Disease 2019 [2, 14]. | |||||||||
YLL contributes in over 51% of the total DALY, so as YLD 48%, meaning that we have impairment in quality of life determined by associated disabilities, and an early mortality (Table 6).
Table 6. The relative share of YLD and YLL in total DALYs. | ||
Sum | % from DALY | |
YLD | 459.04 | 48.57% |
YLL | 486.19 | 51.43% |
DALY | 945.24 | 100% |
Note: YLD - Years lived with disability, YLL - Life years lost as a result of premature mortality, DALY Disability Adjusted Life Years | ||
Composite indicators, such as DALY, is a multipurpose tool for health planning that allows more transparency in showing the impacts of mortality and morbidity of HDV induced liver disease. Thus, health outcomes are potentially highlighted with the aim of making better health-related decisions in the field of current national hepatology.
Discussions
The World Health Organization proposed the goal of eliminating viral hepatitis by 2030 as a target that’s unfortunately still untouched [1]. There are several studies that reflect the actual worldwide epidemiological status of viral hepatopathy, being of particular interest different ways that hepatitis indifferent of etiology HBV (hepatitis B Virus), HCV, HDV or others impacts the patient and society. A prominent leader in the global hepatitis community is Su Wang, scientist reflects the impact of hepatitis and states that one of the most common form of hepatitis is being HBV. In one of the biggest studies Wang et al. mentioned that hepatitis B-related deaths are increasing significantly in countries with high socio-demographic index, such as the UK, the US and Canada, and the social impact of the disease is of substantial interest [5] that’s why the Viral Hepatitis Programs are still considered methods to influence the problem from the root, but we should reconsider the individual, family and society impact of the disease.
The data from China, reflected in a study that aimed to reveal the three-decade dynamics of the natural history of HBV infection in the 1990-2019 period, age-standardized incident rate, age-standardized DALY rate, was used, and the age-standardized mortality rate to quantify the burden of HBV disease per 100,000 person-years. The incidence of cirrhosis and other chronic liver disease decreased significantly between 2010-2015 and remained stable from 2015-2019. The age-standardized incident rate and liver cancer age-standardized death rates remained stable over the period 2010-2019 expect the incidence of HBV-related liver cancer in the period 2019-2044 to decrease by 39.4% also demonstrates, a 36.5% increase in the burden of hepatocellular carcinoma from the total number of DALYs lost due to chronic hepatitis B infection and a 25.8% increase in the total burden of acute viral hepatitis, although there was a decrease of 46.1% in this country on the social impact/hepatic cirrhosis burden [2].
In Brazil, medical scientists have also proposed to evaluate the social impact of liver pathology (referring to hepatitis C, hepatitis B and alcohol-related diseases). Carvalho together with the associations [12] concluded that chronic viral hepatitis and cirrhosis of the liver are responsible for a significant burden in Brazil, mainly affecting men and individuals in the producing age. 57,380 DALYs (30.3 per 100,000 inhabitants) are declared attributable to chronic hepatitis B and cirrhosis due to hepatitis B, with 41,262 DALYs in men. Most of the weight is caused by YLL (47.015 or 24.8/100.000), rather than by YLD (10.365 or 5.5/100.000) [12].
Due to the paucity of information related to HDV, the latter has not been analyzed.
Overall estimates of HBV infection recorded in 2022 report about 258 million chronically infected people [15]. The epidemiological condition in relation to HDV infection is quite robust. Registered in some global regions with orphan disease status, other regions are “enjoying” with intense popularity. The known situation is that HDV is a RNA satellite virus that requires HBV to assemble and introduce de novo viral particles. But as a continuation of the natural progression of the disease, infection with HDV dramatically accelerates the progression of liver disease to liver failure or HCC about 3 times higher than in patients with HBV monoinfection, with a manifest contribution to premature mortality, with a 2 times higher risk [9, 17, 18].
Several studies have used the DALY indicator to estimate the impact of chronic hepatitis B and C in different countries or regions [12-17]. According to the global study of the burden of diseases, a 25% increase in the level of viral hepatitis B burden worldwide to a thousand population, between 1990 and 2010. In the Wang et al study. [5], the authors proposed assessing the burden of the disease through hepatitis B attributable to globally and regionally modifiable risk factors in 204 countries and territories between 1990 and 2019. One third of the total burden of the disease is attributed to smoking status, alcohol consumption and a high body mass index (BMI), which is increasing during the considered period. Although the burden of hepatitis B attributed to tobacco and alcohol consumption decreased, regional disparities in disease burden and time trends differed. Statistically, the study reflects 33.73% of standardized hepatitis B deaths and 34.52% of DALY deaths attributable to smoking status, alcohol consumption and a high BMI. A similar pattern was observed for HCC secondary to HBV, in which about one-third of deaths and DALY were attributed to modifiable lifestyle risk factors [5].
Another study reflecting the state of HBV in China mentions the incidence and declining viral hepatitis DALYs from 1990 to 2016. However, the prevalence still remains at a high level. In 2016, age-standardized DALY rates for hepatitis B were about 9.1/100,000 for mid-high-level regions according to the socio-demographic index 17.4/100,000 for mid-level regions and 56.4/100,000 for medium-low level. Although the age-standardized prevalence rate remains high, the DALY rate fell sharply by 85.5% from 1990 to 2016. This could be partly explained by widely used antiviral therapy. The highest absolute number of DALYs was observed in the 15-49-year-old group in 2016. The highest rate of DALY occurred in men aged 50-69 years and in women aged ≧70 years [13].
The continued increase in the global burden of liver cirrhosis and HCC requires collaborative prevention and control from government, prevention and control departments at multiple levels. Surveillance of patients affected by the HDV continues to be suboptimal, thus masking the real burden of this disease. In the context of poor clinical management, which continues to be a challenge, it remains only to opt for a balanced patient monitoring program, based on the maximum prophylaxis of the installation of complications and slowing down the progression of the disease. As a stage of prevention of HDV infection, we consider justification by promptly implementing measures designed to control HBV. Further efforts are needed, including supplier awareness, patient education and measures to improve the quality of the health system. Let us not forget about the peculiarity that distinguishes HDV, from the bitterness of the rate of evolution of the natural history of the intensely progressive infection. Thus, future medicine in the field of HDV a=induced liver disease relies on the development of surveillance strategies, a phenomenon really depending on strategies of political influencing factors such as Health Policy programs, so in order to direct such programs , we need to prove the existing social impact of the disease in math formulas and stable epidemiological instruments such as DALY, YLD, YLL, their implementation, with expectations of decreasing the social impact of the disease [13, 19-20]. As we mentioned earlier the HDV infection is associated with a higher risk of advanced liver disease in a short period of time, health management and early screening should be strongly applied to this patients [12]. Analyzing the burden of HCC in the enrolled patients, we attest an impairment in men at the productive age. We believe that our study will help to elucidate the characteristics of the national burden of HCC and influence more effective and target prevention strategies.
Health interventions to decrease and control viral hepatitis HDV would cut down the burden of advanced liver disease and reduce the total life years lost to this disease by the community.
Conclusions
Premature mortality associated with viral cirrhosis B and D in the study, with the highest incidence is attested in the age group 30-44 years. Patients aged 45-59 years had the highest YLL index for both women and men with a total YLL of 641.1. Overall, men lost more years of their lives compared to women.
Males exhibited a greater health burden (29.53 age-standardized DALYs per person) than females (25.47 DALYs per person). One DALY representing the loss of the equivalent of one year of full health.
The results obtained oblige us to adapt to the health system, with a strategic planning of medical services and the provision of timely intervention measures, especially for working age groups where the value of the YLL and DALY indicator is increased.
Competing interests
None declared.
Patient consent
Obtained.
Ethics approval
This study was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (No.5 dated 17.06.2022).
Authors’ contribution
AT and OS conceived the study and participated in the study design. EC participated in the study design, recruited eligible patients, completed the study questionnaire, analyzed the data in Excel, performed the statistical analysis, and drafted the manuscript. All authors have read and approved the final version of the article.
Acknowledgements and funding
No external funding.
Authors’ ORCID IDs:
Ecaterina Cebanu – https://orcid.org/0000-0003-0368-1692
Adela Turcanu – https://orcid.org/0000-0002-7684-1768
Octavian Sajin – https://orcid.org/0009-0008-5458-6955
References
World Health Organization. Global hepatitis report 2024: action for access in low-and middle-income countries [Internet]. Geneva: WHO; 2024 [cited 2024 Apr 12]. Available from: https://www.who.int/publications/i/item/9789240091672
Sheena BS, Hiebert L, Han H, Ippolito H, Abbasi-Kangevari M, Abbasi-Kangevari Z, et al. Global, regional, and national burden of hepatitis B, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Gastroenterol Hepatol. 2022;7(9):796-829. doi: 10.1016/S2468-1253(22)00124-8.
Ţurcanu A, Cumpătă V, Tcaciuc E, Pineau P. Profilul hepatitei virale Delta în Republica Moldova – de la transmisia intrafamilială la evoluţia clinică = Delta viral hepatitis profile in Republic of Moldova – between intra-familial transmission and clinical evolution. Mold J Health Sci. 2020;25(4):16-25. Romanian, English.
European Association for the Study of the Liver; Brunetto MR, Ricco G, Negro F, Wedemeyer H, Yurdaydin C, Asselah T, et al. EASL Clinical Practice Guidelines on hepatitis delta virus. J Hepatol. 2023;79(2):433-60. doi: 10.1016/j.jhep.2023.05.001.
Wang M, Yan L, Wang J, Jin Y, Zheng ZJ. Global burden of hepatitis B attributable to modifiable risk factors from 1990 to 2019: a growing contribution and its association with socioeconomic status. Global Health. 2023;19(1):23. doi: 10.1186/s12992-023-00922-z.
Țurcanu A. Evoluția infecției cronice virale Delta – de la hepatită cronică la carcinom hepatocelular [The evolution of chronic Delta viral infection – from chronic hepatitis to hepatocellular carcinoma] [dissertation]. Chisinau: Nicolae Testemitanu SUMPh; 2021. 209 p. Romanian.
Gudima D, Taran N, Tofan-Scutaru L, Ţurcanu A, Hotineanu A, Codreanu I, Peltec A. Liver cirrhosis induced by delta virus in Republic of Moldova: prevalence and mortality on the liver transplant waiting list. J Gastrointestin Liver Dis. 2018;27(Suppl 2):56.
Spînu C, Josanu C, Sajin O, Suveică L, Osoianu I. Studierea și evaluarea impactului social calculat în baza indicatorului DALY produs de infecția cu virusul hepatitei virale B [Study and evaluation of the social impact calculated based on the DALY indicator produced by viral hepatitis B virus infection]. Arta Medica (Chisinau). 2018;67(2):32-35. Romanian.
Stockdale AJ, Kreuels B, Henrion MY, Giorgi E, Kyomuhangi I, de Martel C, Hutin Y, Geretti AM. The global prevalence of hepatitis D virus infection: systematic review and meta-analysis. J Hepatol. 2020;73(3):523-532. doi: 10.1016/j.jhep.2020.04.008.
Razavi-Shearer D, Child H, Razavi-Shearer K, Voeller A, Razavi H, Buti M, Tacke F, Terrault N, Zeuzem S, Abbas Z, Aghemo A. Adjusted estimate of the prevalence of hepatitis delta virus in 25 countries and territories. J Hepatol. 2024;80(2):232-242. doi: 10.1016/j.jhep.2023.10.043.
Ţurcanu A. Conceptul de cancer precoce la pacienții cu hepatopatie cronică virală B, C şi Delta [The concept of early cancer in patients with chronic viral hepatopathy B, C and Delta]. Bull Acad Sci Mold. Med Sci. 2020;68(4):136-145.
de Carvalho JR, Villela-Nogueira CA, Perez RM, Portugal FB, Flor LS, Campos MR, Schramm JM. Burden of chronic viral hepatitis and liver cirrhosis in Brazil – the Brazilian Global Burden of Disease Study. Ann Hepatol. 2018;16(6):893-900. doi: 10.5604/01.3001.0010.5280.
Li M, Wang ZQ, Zhang L, Zheng H, Zhou MG, Liu DW. Burden of viral hepatitis caused by specific aetiologies in China, 1990-2016: findings from the GBD 2016. BMC Public Health. 2020;20(1):1461. doi: 10.1186/s12889-020-09533-4.
Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204-22. doi: 10.1016/S0140-6736(20)30925-9.
Razavi-Shearer D, Gamkrelidze I, Pan C, Jia J, Berg T, Gray R, et al. Global prevalence, cascade of care, and prophylaxis coverage of hepatitis B in 2022: a modelling study. Lancet Gastroenterol Hepatol. 2023;8(10):879-907. doi: 10.1016/S2468-1253(23)00197-8.
Penina O. Regional mortality disparities in the Republic of Moldova. Chișinău: Medicina; 2022. 116 p.
Razavi-Shearer D, Child H, Razavi-Shearer K, Voeller A, Razavi H, Buti M, et al. Adjusted estimate of the prevalence of hepatitis delta virus in 25 countries and territories. J Hepatol. 2024;80(2):232-42. doi: 10.1016/j.jhep.2023.10.043.
Kamal H, Fornes R, Simin J, Stål P, Duberg AS, Brusselaers N, Aleman S. Risk of hepatocellular carcinoma in hepatitis B and D virus co‐infected patients: a systematic review and meta‐analysis of longitudinal studies. J Viral Hepat. 2021;28(10):1431-42. doi: 10.1111/jvh.13577.
Lin L, Yan L, Liu Y, Qu C, Ni J, Li H. The burden and trends of primary liver cancer caused by specific etiologies from 1990 to 2017 at the global, regional, national, age, and sex level results from the global burden of disease study 2017. Liver Cancer. 2020;9(5):563-82. doi: 10.1159/000508568.
Wyper GM, Devleesschauwer B, Mathers CD, McDonald SA, Speybroeck N. Years of life lost methods must remain fully equitable and accountable. Eur J Epidemiol. 2022;37(2):215-216. doi: 10.1007/s10654-022-00846-9.